

International versus national growth charts for identifying small and large-for-gestational age newborns: A population-based study in 15 European countries
- PMID: 34557855
- PMCID: PMC8454535
- DOI: 10.1016/j.lanepe.2021.100167
International versus national growth charts for identifying small and large-for-gestational age newborns: A population-based study in 15 European countries
Abstract
Background: To inform the on-going debate about the use of universal prescriptive versus national intrauterine growth charts, we compared perinatal mortality for small and large-for-gestational-age (SGA/LGA) infants according to international and national charts in Europe.
Methods: We classified singleton births from 33 to 42 weeks of gestation in 2010 and 2014 from 15 countries (N = 1,475,457) as SGA (birthweight <10th percentile) and LGA (>90th percentile) using the international Intergrowth-21st newborn standards and national charts based on the customised charts methodology. We computed sex-adjusted odds ratios (aOR) for stillbirth, neonatal and extended perinatal mortality by this classification using multilevel models.
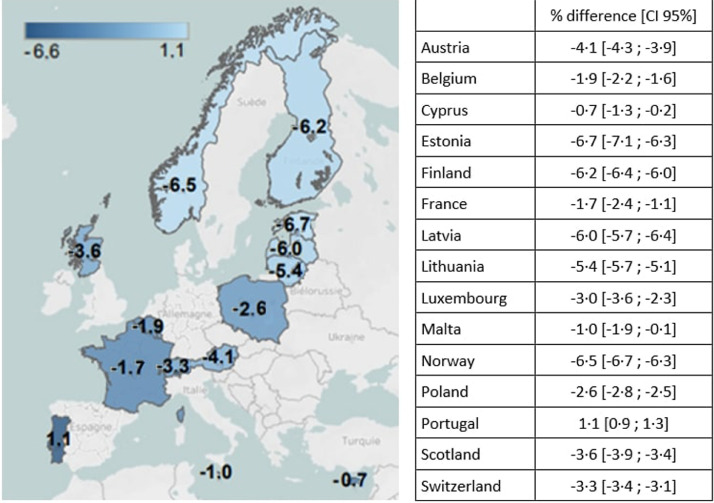
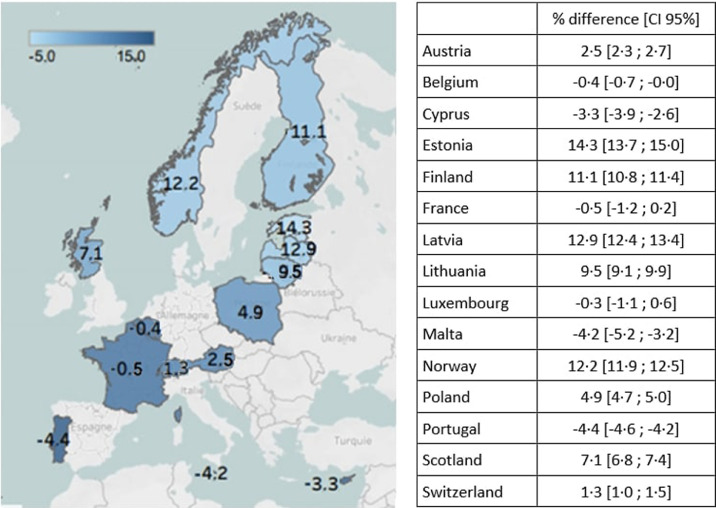
Findings: SGA and LGA prevalence using national charts were near 10% in all countries, but varied according to international charts with a north to south gradient (3.0% to 10.1% and 24.9% to 8.0%, respectively). Compared with appropriate for gestational age (AGA) infants by both charts, risk of perinatal mortality was increased for SGA by both charts (aOR[95% confidence interval (CI)]=6.1 [5.6-6.7]) and infants reclassified by international charts from SGA to AGA (2.7 [2.3-3.1]), but decreased for those reclassified from AGA to LGA (0.6 [0.4-0.7]). Results were similar for stillbirth and neonatal death.
Interpretation: Using international instead of national charts in Europe could lead to growth restricted infants being reclassified as having normal growth, while infants with low risks of mortality could be reclassified as having excessive growth.
Funding: InfAct Joint Action, CHAFEA Grant n°801,553 and EU/EFPIA Innovative Medicines Initiative 2 Joint Undertaking ConcePTION grant n°821,520. AH received a PhD grant from EHESP.
Keywords: fetal growth; fetal growth charts; large for gestational age; small for gestational age.
© 2021 The Authors.
Conflict of interest statement
No conflict of interest to disclose.
Figures
References
-
- Vayssière C., Sentilhes L., Ego A., Bernard C., Cambourieu D., Flamant C. Fetal growth restriction and intra-uterine growth restriction: guidelines for clinical practice from the French College of Gynaecologists and Obstetricians. Eur J Obstet Gynecol Reprod Biol. 2015 Oct;193:10–18. - PubMed
-
- ACOG Practice Bulletin No. 204: fetal growth restriction. Obstet Gynecol. 2019;133(2):e97–109. - PubMed
-
- Flenady V., Koopmans L., Middleton P., Frøen J.F., Smith G.C., Gibbons K. Major risk factors for stillbirth in high-income countries: a systematic review and meta-analysis. Lancet. 2011 Apr 16;377(9774):1331–1340. - PubMed
-
- Baschat A.A., Viscardi R.M., Hussey-Gardner B., Hashmi N., Harman C. Infant neurodevelopment following fetal growth restriction: relationship with antepartum surveillance parameters. Ultrasound Obstet Gynecol. 2009 Jan;33(1):44–50. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
