

Outcomes of Elderly Patients Undergoing Left Atrial Appendage Closure
- PMID: 34558289
- PMCID: PMC8649147
- DOI: 10.1161/JAHA.121.021973
Outcomes of Elderly Patients Undergoing Left Atrial Appendage Closure
Abstract
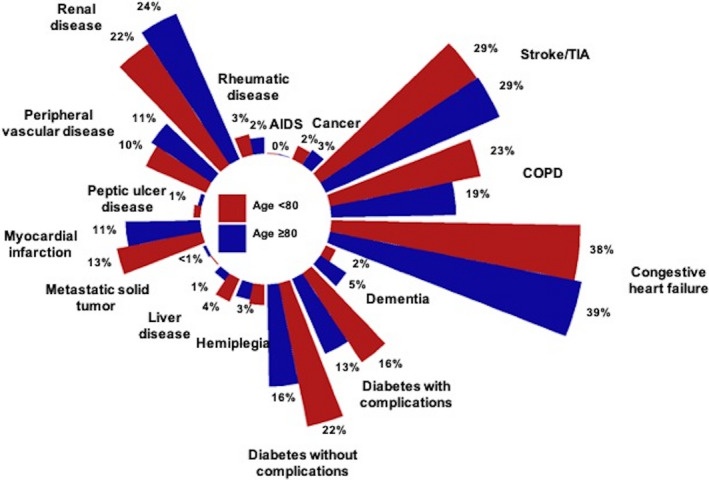
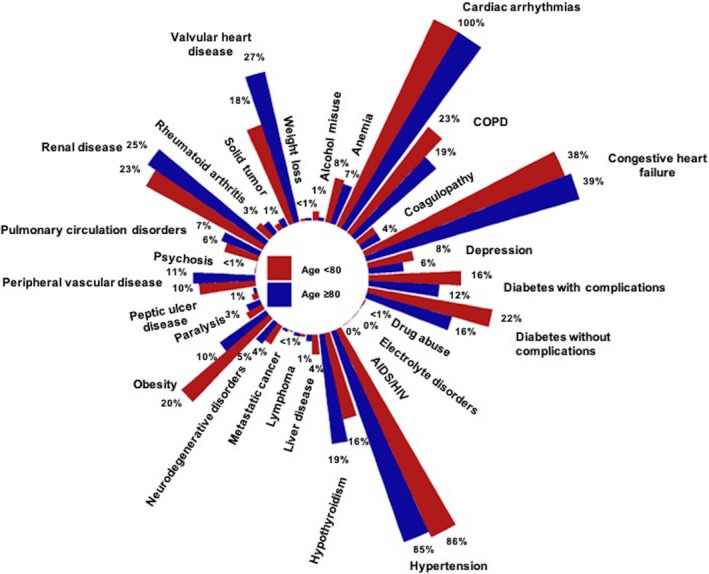
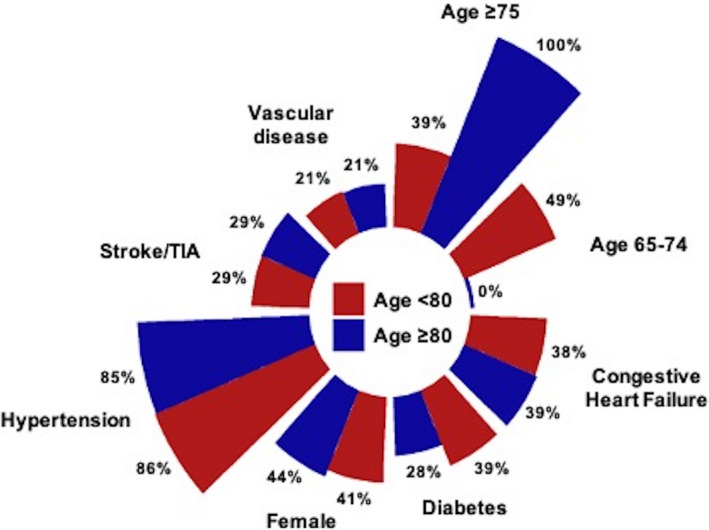
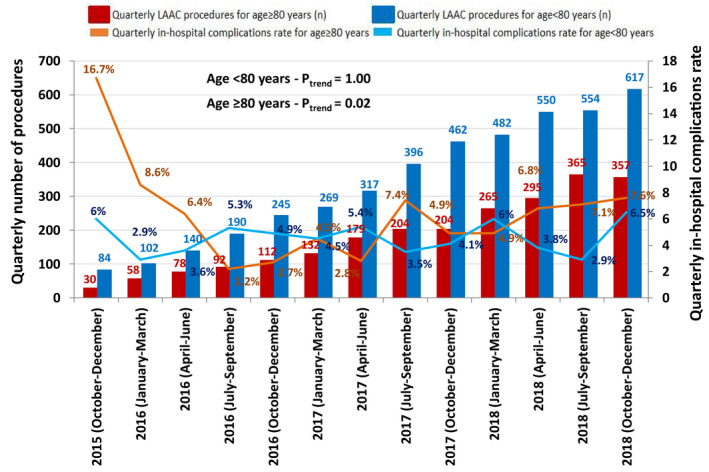
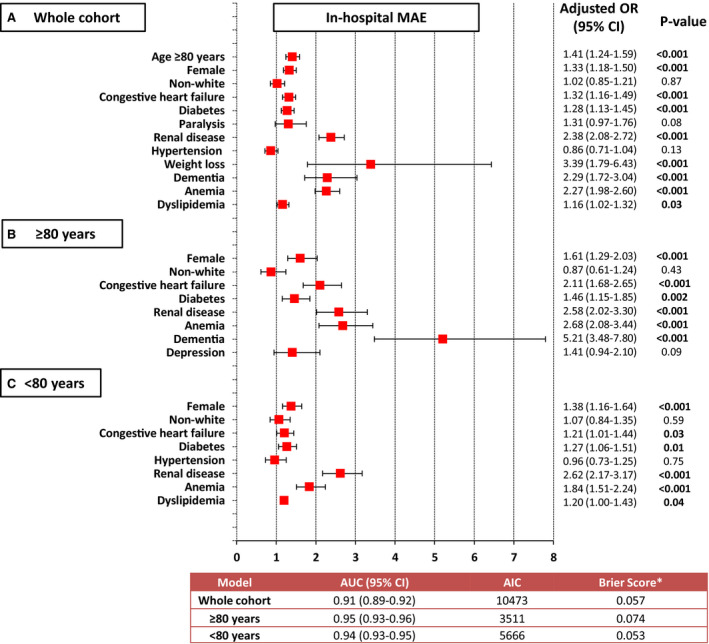
Background Elderly patients have a higher burden of comorbidities that influence clinical outcomes. We aimed to compare in-hospital outcomes in patients ≥80 years old to younger patients, and to determine the factors associated with increased risk of major adverse events (MAE) after left atrial appendage closure. Methods and Results The National Inpatient Sample was used to identify discharges after left atrial appendage closure between October 2015 and December 2018. The primary outcome was in-hospital MAE defined as the composite of postprocedural bleeding, vascular and cardiac complications, acute kidney injury, stroke, and death. A total of 6779 hospitalizations were identified, of which, 2371 (35%) were ≥80 years old and 4408 (65%) were <80 years old. Patients ≥80 years old experienced a higher rate of MAE compared with those aged <80 years old (6.0% versus 4.6%, P=0.01), and this difference was driven by a numerically higher rate of cardiac complications (2.4% versus 1.8%, P=0.09) and death (0.3% versus 0.1%, P=0.05) among individuals ≥80 years old. In patients ≥80 years old, higher odds of in-hospital MAE were observed in women (1.61-fold), and those with preprocedural congestive heart failure (≈2-fold), diabetes (≈1.5-fold), renal disease (≈2.6-fold), anemia (≈2.7-fold), and dementia (≈5-fold). In patients <80 years old, a higher risk of in-hospital MAE was encountered among women (≈1.4-fold) and those with diabetes (≈1.3-fold), renal disease (≈2.6-fold), anemia (≈2-fold), and dyslipidemia (≈1.2-fold). Conclusions Patients ≥80 years old had higher rates of in-hospital MAE compared with patients aged <80 years old. Female sex and the presence of heart failure, diabetes, renal disease, and anemia were factors associated with in-hospital MAE among both groups.
Keywords: anticoagulation; atrial fibrillation; comorbidities; elderly; left atrial appendage closure; octogenarians; stroke.
Conflict of interest statement
Dr Holmes is on the Advisory Board for Boston Scientific, unpaid. The remaining authors have no disclosures to report.
Figures
References
-
- Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor‐based approach: the Euro Heart Survey on Atrial Fibrillation. Chest. 2010;137:263–272. doi: 10.1378/chest.09-1584 - DOI - PubMed
-
- Dang G, Jahangir I, Sra J, Tajik AJ, Jahangir A. Atrial fibrillation and stroke in elderly patients. J Patient Cent Res Rev. 2016;3:217–229. doi: 10.17294/2330-0698.1409 - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
