

Prediction Model Performance With Different Imputation Strategies: A Simulation Study Using a North American ICU Registry
- PMID: 34560774
- PMCID: PMC8719509
- DOI: 10.1097/PCC.0000000000002835
Prediction Model Performance With Different Imputation Strategies: A Simulation Study Using a North American ICU Registry
Abstract
Objectives: To evaluate the performance of pragmatic imputation approaches when estimating model coefficients using datasets with varying degrees of data missingness.
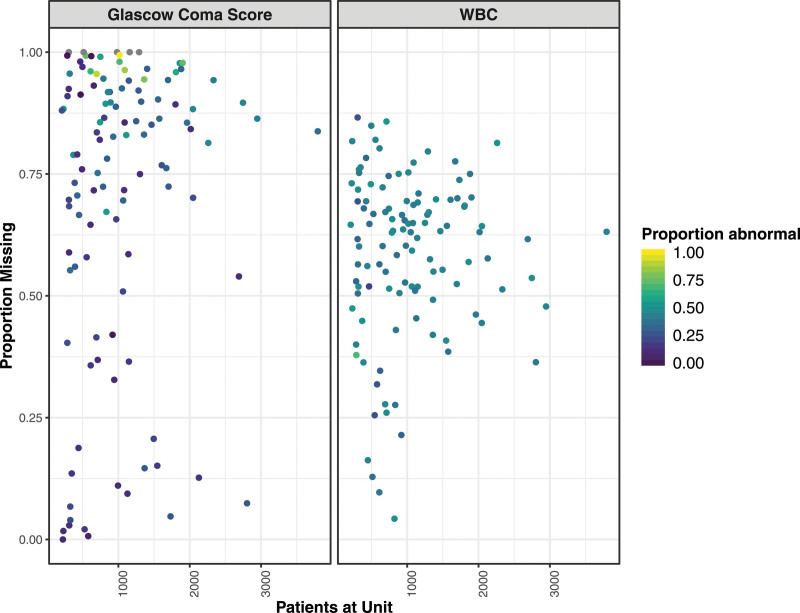
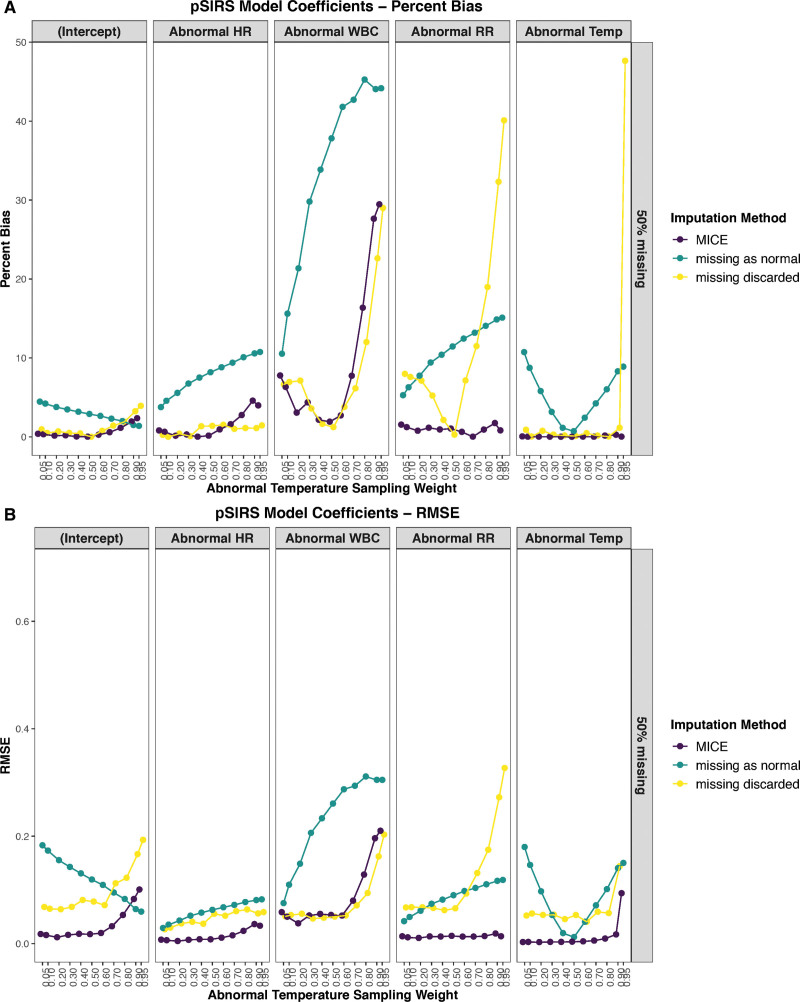
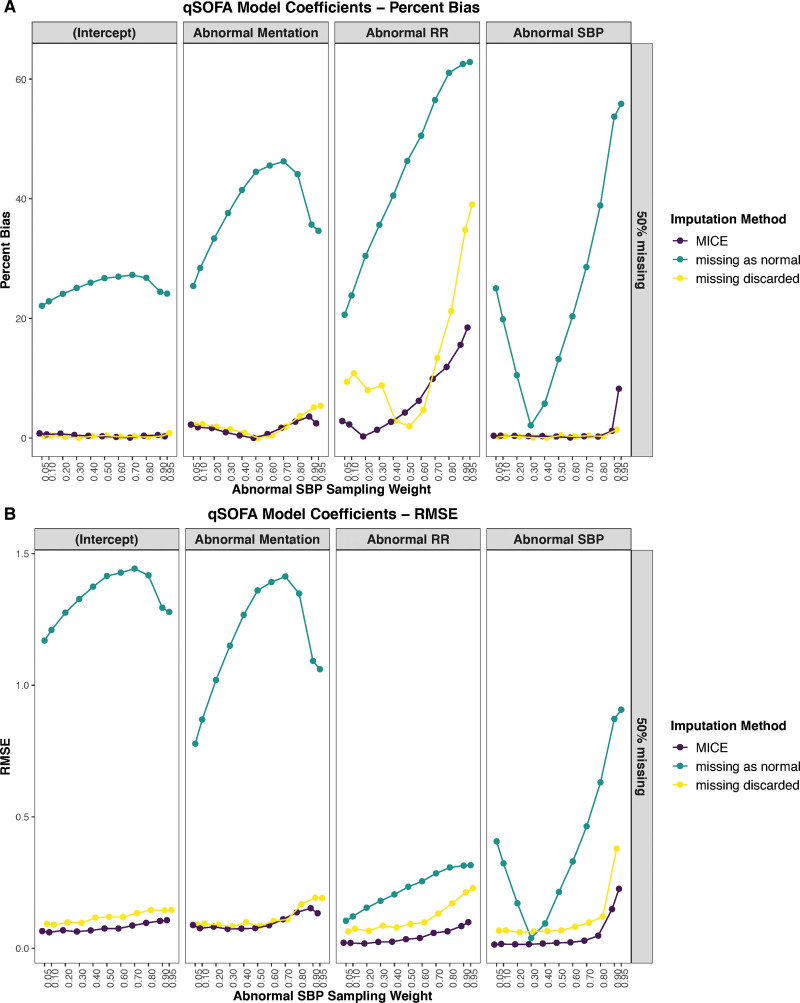
Design: Performance in predicting observed mortality in a registry dataset was evaluated using simulations of two simple logistic regression models with age-specific criteria for abnormal vital signs (mentation, systolic blood pressure, respiratory rate, WBC count, heart rate, and temperature). Starting with a dataset with complete information, increasing degrees of biased missingness of WBC and mentation were introduced, depending on the values of temperature and systolic blood pressure, respectively. Missing data approaches evaluated included analysis of complete cases only, assuming missing data are normal, and multiple imputation by chained equations. Percent bias and root mean square error, in relation to parameter estimates obtained from the original data, were evaluated as performance indicators.
Setting: Data were obtained from the Virtual Pediatric Systems, LLC, database (Los Angeles, CA), which provides clinical markers and outcomes in prospectively collected records from 117 PICUs in the United States and Canada.
Patients: Children admitted to a participating PICU in 2017, for whom all required data were available.
Interventions: None.
Measurements and main results: Simulations demonstrated that multiple imputation by chained equations is an effective strategy and that even a naive implementation of multiple imputation by chained equations significantly outperforms traditional approaches: the root mean square error for model coefficients was lower using multiple imputation by chained equations in 90 of 99 of all simulations (91%) compared with discarding cases with missing data and lower in 97 of 99 (98%) compared with models assuming missing values are in the normal range. Assuming missing data to be abnormal was inferior to all other approaches.
Conclusions: Analyses of large observational studies are likely to encounter the issue of missing data, which are likely not missing at random. Researchers should always consider multiple imputation by chained equations (or similar imputation approaches) when encountering even only small proportions of missing data in their work.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.
Conflict of interest statement
Dr. Steif received funding from the University of British Columbia (UBC). Dr. Brant received support for article research from the British Columbia Children’s Hospital Research Institute. Dr. Sreepada’s institution received funding from Mitacs Postdoctoral Fellowship. Dr. Murthy holds a Research Chair from Health Research Foundation and Innovative Medicines Canada. Dr. Görges’ institution received funding from the Natural Sciences and Engineering Research Council of Canada, the Canadian Institutes of Health Research, the Juvenile Diabetes Research Foundation, and the British Columbia Children’s Hospital Research Institute; he received funding from the Michael Smith Foundation for Health Research; he disclosed he is party to a licensing agreement between UBC and NeuroWave Systems for unrelated work, that he was a director for the Society for Technology in Anesthesia, and a principal investigator and coinvestigator for Canada’s Digital Technology Supercluster projects. Mr. West has disclosed that he does not have any potential conflicts of interest.
Figures
References
-
- Peters C, Murthy S, Brant R, et al. . Mortality risk using a pediatric quick sequential (sepsis-related) organ failure assessment varies with vital sign thresholds. Pediatr Crit Care Med. 2018; 19:e394–e402 - PubMed
-
- Görges M, Peters C, Murthy S, et al. . External validation of the “quick” pediatric logistic organ dysfunction-2 score using a large North American cohort of critically ill children with suspected infection. Pediatr Crit Care Med. 2018; 19:1114–1119 - PubMed
-
- Slater A, Shann F, Pearson G; Paediatric Index of Mortality (PIM) Study Group. PIM2: A revised version of the Paediatric Index of Mortality. Intensive Care Med. 2003; 29:278–285 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
