

Serological responses to SARS-CoV-2 following non-hospitalised infection: clinical and ethnodemographic features associated with the magnitude of the antibody response
- PMID: 34561239
- PMCID: PMC8474079
- DOI: 10.1136/bmjresp-2020-000872
Serological responses to SARS-CoV-2 following non-hospitalised infection: clinical and ethnodemographic features associated with the magnitude of the antibody response
Abstract
Objective: To determine clinical and ethnodemographic correlates of serological responses against the SARS-CoV-2 spike glycoprotein following mild-to-moderate COVID-19.
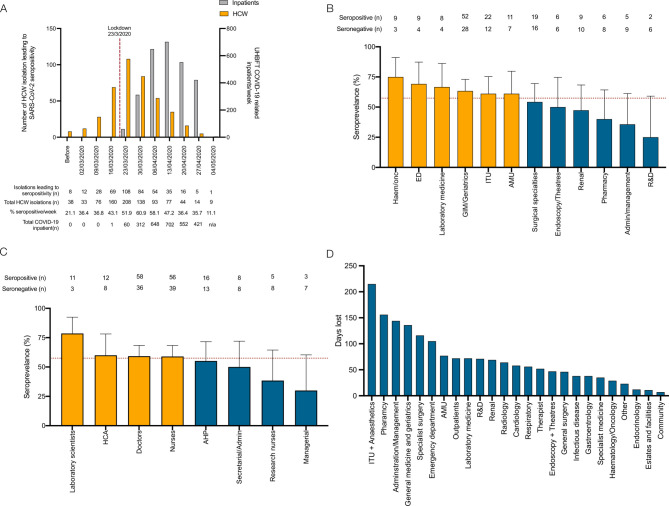
Design: A retrospective cohort study of healthcare workers who had self-isolated due to COVID-19.
Setting: University Hospitals Birmingham NHS Foundation Trust, UK (UHBFT).
Participants: 956 healthcare workers were recruited by open invitation via UHBFT trust email and social media between 27 April 2020 and the 8 June 2020.
Intervention: Participants volunteered a venous blood sample that was tested for the presence of anti-SARS-CoV-2 spike glycoprotein antibodies. Results were interpreted in the context of the symptoms of their original illness and ethnodemographic variables.
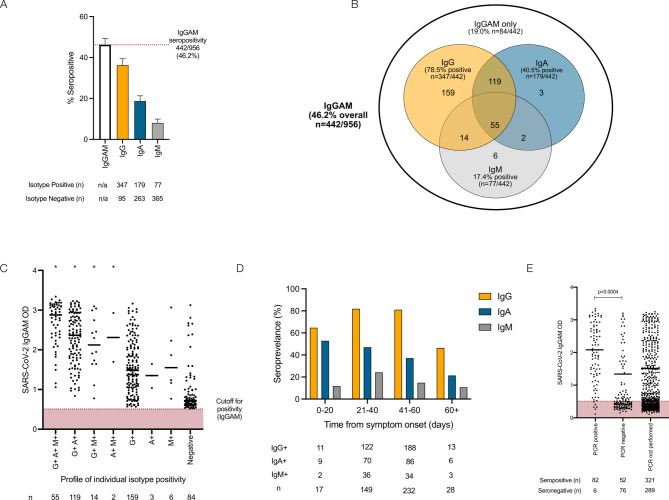
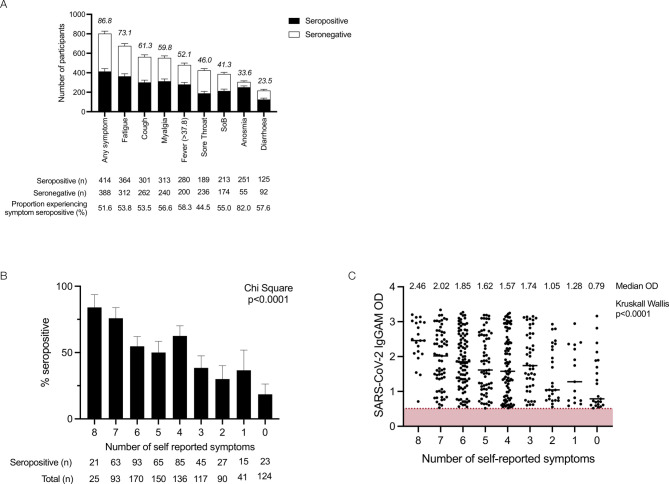
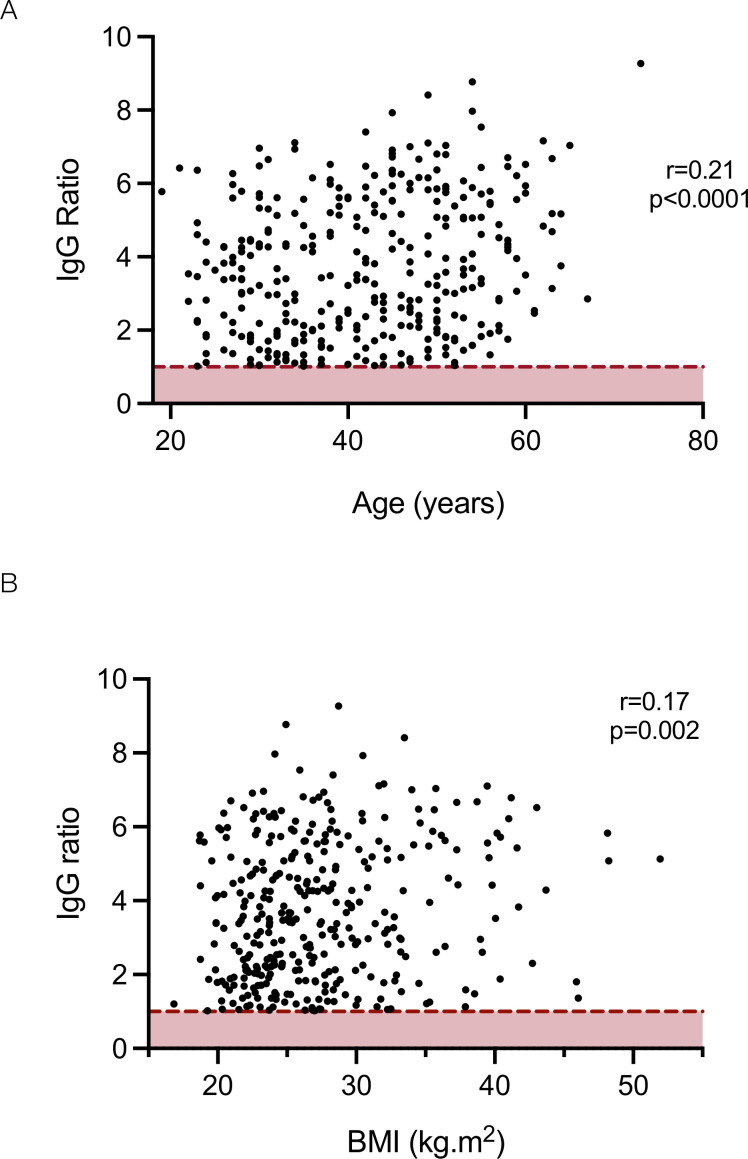
Results: Using an assay that simultaneously measures the combined IgG, IgA and IgM response against the spike glycoprotein (IgGAM), the overall seroprevalence within this cohort was 46.2% (n=442/956). The seroprevalence of immunoglobulin isotypes was 36.3%, 18.7% and 8.1% for IgG, IgA and IgM, respectively. IgGAM identified serological responses in 40.6% (n=52/128) of symptomatic individuals who reported a negative SARS-CoV-2 PCR test. Increasing age, non-white ethnicity and obesity were independently associated with greater IgG antibody response against the spike glycoprotein. Self-reported fever and fatigue were associated with greater IgG and IgA responses against the spike glycoprotein. The combination of fever and/or cough and/or anosmia had a positive predictive value of 92.3% for seropositivity in self-isolating individuals a time when Wuhan strain SARS-CoV-2 was predominant.
Conclusions and relevance: Assays employing combined antibody detection demonstrate enhanced seroepidemiological sensitivity and can detect prior viral exposure even when PCR swabs have been negative. We demonstrate an association between known ethnodemographic risk factors associated with mortality from COVID-19 and the magnitude of serological responses in mild-to-moderate disease.
Keywords: COVID-19; clinical epidemiology; respiratory infection.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: MTD reports personal fees from Abingdon Health, outside the submitted work.
Figures
Update of
-
Serological responses to SARS-CoV-2 following non-hospitalised infection: clinical and ethnodemographic features associated with the magnitude of the antibody response.medRxiv [Preprint]. 2020 Nov 16:2020.11.12.20230763. doi: 10.1101/2020.11.12.20230763. medRxiv. 2020. Update in: BMJ Open Respir Res. 2021 Sep;8(1):e000872. doi: 10.1136/bmjresp-2020-000872. PMID: 33236029 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous