

Artificial intelligence system reduces false-positive findings in the interpretation of breast ultrasound exams
- PMID: 34561440
- PMCID: PMC8463596
- DOI: 10.1038/s41467-021-26023-2
Artificial intelligence system reduces false-positive findings in the interpretation of breast ultrasound exams
Abstract
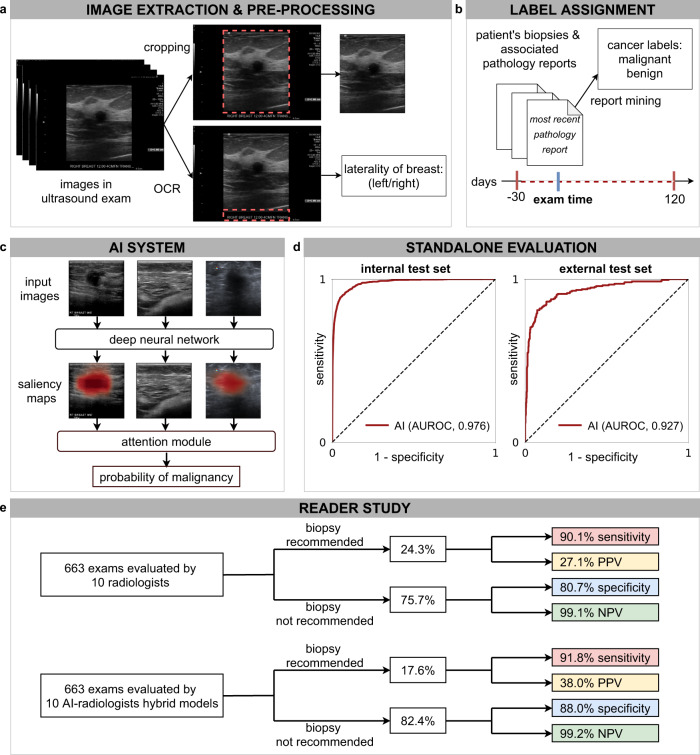
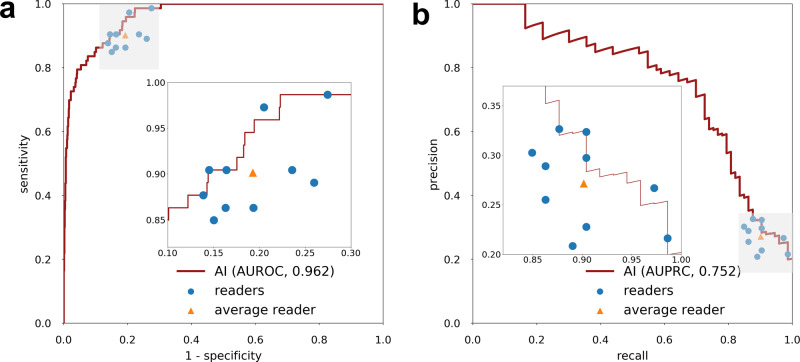
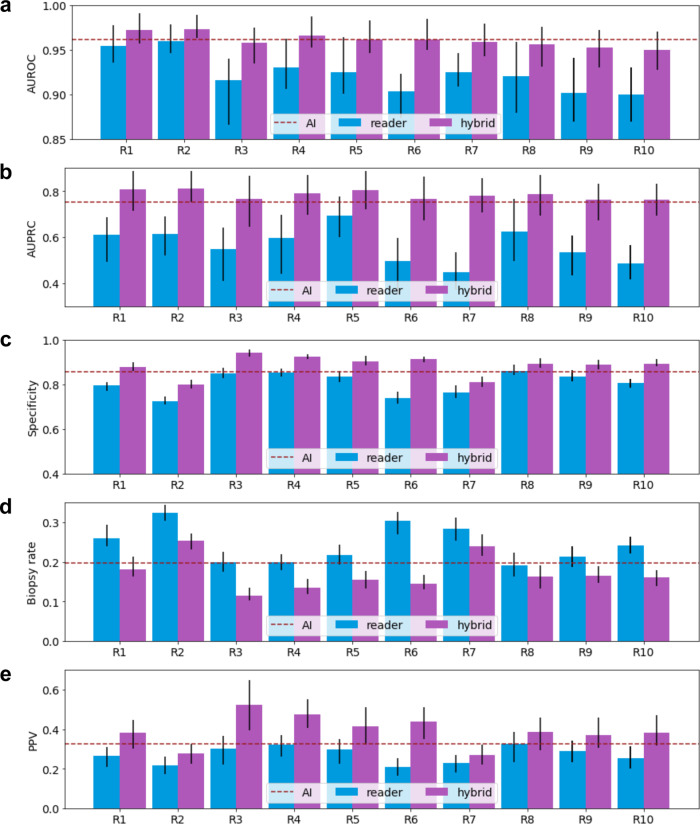
Though consistently shown to detect mammographically occult cancers, breast ultrasound has been noted to have high false-positive rates. In this work, we present an AI system that achieves radiologist-level accuracy in identifying breast cancer in ultrasound images. Developed on 288,767 exams, consisting of 5,442,907 B-mode and Color Doppler images, the AI achieves an area under the receiver operating characteristic curve (AUROC) of 0.976 on a test set consisting of 44,755 exams. In a retrospective reader study, the AI achieves a higher AUROC than the average of ten board-certified breast radiologists (AUROC: 0.962 AI, 0.924 ± 0.02 radiologists). With the help of the AI, radiologists decrease their false positive rates by 37.3% and reduce requested biopsies by 27.8%, while maintaining the same level of sensitivity. This highlights the potential of AI in improving the accuracy, consistency, and efficiency of breast ultrasound diagnosis.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
