

Clinical performance of methylation as a biomarker for cervical carcinoma in situ and cancer diagnosis: A worldwide study
- PMID: 34562270
- PMCID: PMC8627461
- DOI: 10.1002/ijc.33815
Clinical performance of methylation as a biomarker for cervical carcinoma in situ and cancer diagnosis: A worldwide study
Abstract
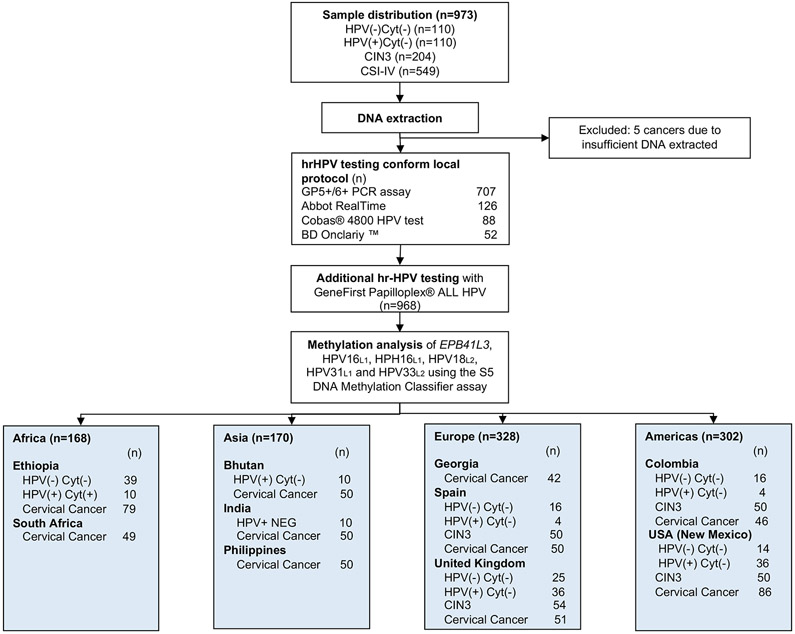
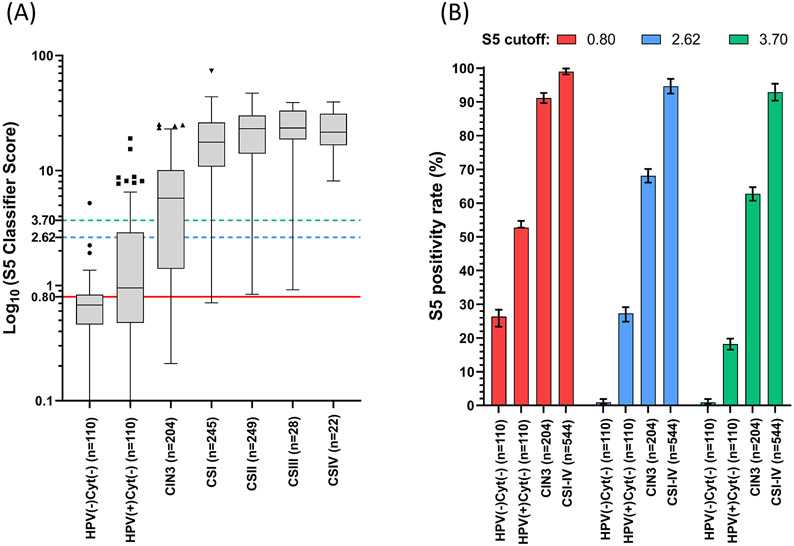
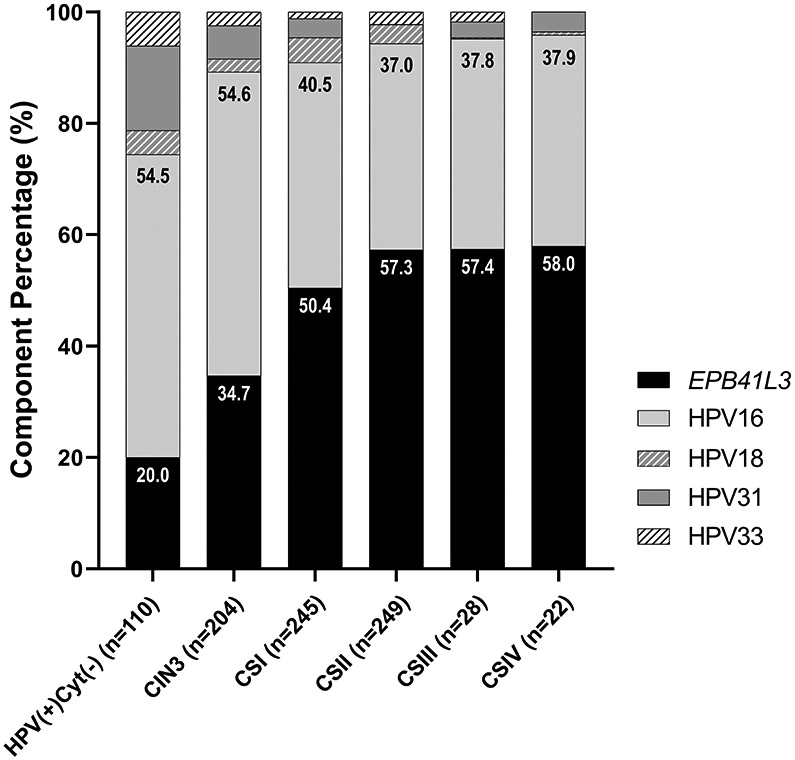
The shift towards primary human papillomavirus (HPV)-based screening has necessitated the search for a secondary triage test that provides sufficient sensitivity to detect high-grade cervical intraepithelial neoplasia (CIN) and cancer, but also brings an improved specificity to avoid unnecessary clinical work and colposcopy referrals. We evaluated the performance of the previously described DNA-methylation test (S5) in detecting CIN3 and cancers from diverse geographic settings in high-, medium- and low-income countries, using the cut-off of 0.80 and exploratory cut-offs of 2.62 and 3.70. Assays were performed using exfoliated cervical specimens (n = 808) and formalin-fixed biopsies (n = 166) from women diagnosed with cytology-negative results (n = 220), CIN3 (n = 204) and cancer stages I (n = 245), II (n = 249), III (n = 28) and IV (n = 22). Methylation increased proportionally with disease severity (Cuzick test for trend, P < .0001). S5 accurately separated women with negative-histology from CIN3 or cancer (P < .0001). At the 0.80 cut-off, 543/544 cancers were correctly identified as S5 positive (99.81%). At cut-off 3.70, S5 showed a sensitivity of 95.77% with improved specificity. The S5 odds ratios of women negative for cervical disease vs CIN3+ were significantly higher than for HPV16/18 genotyping at all cut-offs (all P < .0001). At S5 cut-off 0.80, 96.15% of consistently high-risk human papillomavirus (hrHPV)-negative cancers (tested with multiple hrHPV-genotyping assay) were positive by S5. These cancers may have been missed in current primary hrHPV-screening programmes. The S5 test can accurately detect CIN3 and malignancy irrespective of geographic context and setting. The test can be used as a screening and triage tool. Adjustment of the S5 cut-off can be performed considering the relative importance given to sensitivity vs specificity.
Keywords: DNA methylation; HPV; cancer screening; cervical cancer; high-risk human papillomavirus; molecular triage; triage.
© 2021 The Authors. International Journal of Cancer published by John Wiley & Sons Ltd on behalf of UICC.
Conflict of interest statement
Conflict Interest
KC reports her employer having received research funding or gratis consumables to support research from the following in the last 3 years: Cepheid, Furoimmun, Genefirst, Selfscreen, Hiantis, Seegene, Roche, Abbott, Hologic. CMW reports receiving the following outside the submitted work: cooperative agreements and grants from the US National Institutes of Health for research on cancer prevention and sexually transmitted infections, reagents and equipment from Roche Molecular Systems, Roche/Ventana Medical Systems, Hologic and Genera Biosystems, research funding from Hologic and Becton Dickinson (BD) and personal fees from BD. The other authors declare no conflict of interest.
Figures
References
-
- Allen-Leigh B, Uribe-Zúñiga P, León-Maldonado L, Brown BJ, Lörincz A, Salmeron J, Lazcano-Ponce E. Barriers to HPV self-sampling and cytology among low-income indigenous women in rural areas of a middle-income setting: a qualitative study. BMC Cancer. 2017. November 9;17(1):734. doi: 10.1186/s12885-017-3723-5. - DOI - PMC - PubMed
-
- Cuschieri K, Ronco G, Lorincz A, Smith L, Ogilvie G, Mirabello L, Carozzi F, Cubie H, Wentzensen N, Snijders P, Arbyn M, Monsonego J, Franceschi S. Eurogin roadmap 2017: Triage strategies for the management of HPV-positive women in cervical screening programs. Int J Cancer. 2018. August 15;143(4):735–745. doi: 10.1002/ijc.31261. - DOI - PubMed
