

Estimated effect of increased diagnosis, treatment, and control of diabetes and its associated cardiovascular risk factors among low-income and middle-income countries: a microsimulation model
- PMID: 34562369
- PMCID: PMC8526364
- DOI: 10.1016/S2214-109X(21)00340-5
Estimated effect of increased diagnosis, treatment, and control of diabetes and its associated cardiovascular risk factors among low-income and middle-income countries: a microsimulation model
Erratum in
-
Correction to Lancet Glob Health 2021; 9: e1539-52.Lancet Glob Health. 2022 Feb;10(2):e185. doi: 10.1016/S2214-109X(21)00585-4. Epub 2021 Dec 8. Lancet Glob Health. 2022. PMID: 34895516 Free PMC article. No abstract available.
Abstract
Background: Given the increasing prevalence of diabetes in low-income and middle-income countries (LMICs), we aimed to estimate the health and cost implications of achieving different targets for diagnosis, treatment, and control of diabetes and its associated cardiovascular risk factors among LMICs.
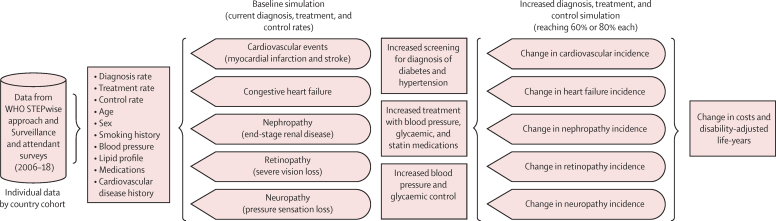
Methods: We constructed a microsimulation model to estimate disability-adjusted life-years (DALYs) lost and health-care costs of diagnosis, treatment, and control of blood pressure, dyslipidaemia, and glycaemia among people with diabetes in LMICs. We used individual participant data-specifically from the subset of people who were defined as having any type of diabetes by WHO standards-from nationally representative, cross-sectional surveys (2006-18) spanning 15 world regions to estimate the baseline 10-year risk of atherosclerotic cardiovascular disease (defined as fatal and non-fatal myocardial infarction and stroke), heart failure (ejection fraction of <40%, with New York Heart Association class III or IV functional limitations), end-stage renal disease (defined as an estimated glomerular filtration rate <15 mL/min per 1·73 m2 or needing dialysis or transplant), retinopathy with severe vision loss (<20/200 visual acuity as measured by the Snellen chart), and neuropathy with pressure sensation loss (assessed by the Semmes-Weinstein 5·07/10 g monofilament exam). We then used data from meta-analyses of randomised controlled trials to estimate the reduction in risk and the WHO OneHealth tool to estimate costs in reaching either 60% or 80% of diagnosis, treatment initiation, and control targets for blood pressure, dyslipidaemia, and glycaemia recommended by WHO guidelines. Costs were updated to 2020 International Dollars, and both costs and DALYs were computed over a 10-year policy planning time horizon at a 3% annual discount rate.
Findings: We obtained data from 23 678 people with diabetes from 67 countries. The median estimated 10-year risk was 10·0% (IQR 4·0-18·0) for cardiovascular events, 7·8% (5·1-11·8) for neuropathy with pressure sensation loss, 7·2% (5·6-9·4) for end-stage renal disease, 6·0% (4·2-8·6) for retinopathy with severe vision loss, and 2·6% (1·2-5·3) for congestive heart failure. A target of 80% diagnosis, 80% treatment, and 80% control would be expected to reduce DALYs lost from diabetes complications from a median population-weighted loss to 1097 DALYs per 1000 population over 10 years (IQR 1051-1155), relative to a baseline of 1161 DALYs, primarily from reduced cardiovascular events (down from a median of 143 to 117 DALYs per 1000 population) due to blood pressure and statin treatment, with comparatively little effect from glycaemic control. The target of 80% diagnosis, 80% treatment, and 80% control would be expected to produce an overall incremental cost-effectiveness ratio of US$1362 per DALY averted (IQR 1304-1409), with the majority of decreased costs from reduced cardiovascular event management, counterbalanced by increased costs for blood pressure and statin treatment, producing an overall incremental cost-effectiveness ratio of $1362 per DALY averted (IQR 1304-1409).
Interpretation: Reducing complications from diabetes in LMICs is likely to require a focus on scaling up blood pressure and statin medication treatment initiation and blood pressure medication titration rather than focusing on increasing screening to increase diabetes diagnosis, or a glycaemic treatment and control among people with diabetes.
Funding: None.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests SB reports grants from the US National Institutes of Health (NIH) and US Centers for Disease Control and Prevention; consulting fees from the Clinton Health Access Initiative and University of California San Francisco; patents pending for a multi-model patient outreach system; unpaid leadership roles at La Scuola International School and Columbia University Global Research Analytics for Population Health; and stock options at Collective Health, outside the submitted work. DF reports volunteer affiliations with Wuqu' Kawoq and GlucoSalud, outside the submitted work. RA reports contracts with Novo Nordisk, outside the submitted work. TB reports grants from the NIH–National Institute of Allergy and Infectious Diseases, NIH–National Institute on Aging, NIH, National Institute of Child Health and Human Development, Wellcome, Alexander von Humboldt Foundation, UNAIDS, German Research Foundation, European Union, German Federal Ministry of Education and Research, German Federal Ministry of Environment, Nature Conservation and Nuclear Safety, German Federal Ministry of Health, KfW, Else Kröner Foundation, African Academy of Science, European and Developing Countries Clinical Trials Partnership, and the Bill & Melinda Gates Foundation. All other authors declare no competing interests.
Figures

Comment in
-
Achieving sensible targets for a diabetes care cascade in LMICs.Lancet Glob Health. 2021 Nov;9(11):e1481-e1482. doi: 10.1016/S2214-109X(21)00403-4. Epub 2021 Sep 22. Lancet Glob Health. 2021. PMID: 34562370 No abstract available.
References
-
- International Diabetes Federation IDF Diabetes Atlas 9th edn 2019. 2019. https://www.diabetesatlas.org/en/sections/worldwide-toll-of-diabetes.html
-
- UN Statistics Division SDG indicators: metadata repository. 2021. https://unstats.un.org/sdgs/metadata/?Text=&Goal=3&Target=3.4
-
- WHO WHO announces the Global Diabetes Compact. 2020. https://www.who.int/news/item/17-11-2020-who-announces-the-global-diabet...
-
- Atun R, Davies JI, Gale EAM. Diabetes in sub-Saharan Africa: from clinical care to health policy. Lancet Diabetes Endocrinol. 2017;5:622–667. - PubMed
