

Antibiotics for lower respiratory tract infection in children presenting in primary care in England (ARTIC PC): a double-blind, randomised, placebo-controlled trial
- PMID: 34562391
- PMCID: PMC8542731
- DOI: 10.1016/S0140-6736(21)01431-8
Antibiotics for lower respiratory tract infection in children presenting in primary care in England (ARTIC PC): a double-blind, randomised, placebo-controlled trial
Abstract
Background: Antibiotic resistance is a global public health threat. Antibiotics are very commonly prescribed for children presenting with uncomplicated lower respiratory tract infections (LRTIs), but there is little evidence from randomised controlled trials of the effectiveness of antibiotics, both overall or among key clinical subgroups. In ARTIC PC, we assessed whether amoxicillin reduces the duration of moderately bad symptoms in children presenting with uncomplicated (non-pneumonic) LRTI in primary care, overall and in key clinical subgroups.
Methods: ARTIC PC was a double-blind, randomised, placebo-controlled trial done at 56 general practices in England. Eligible children were those aged 6 months to 12 years presenting in primary care with acute uncomplicated LRTI judged to be infective in origin, where pneumonia was not suspected clinically, with symptoms for less than 21 days. Patients were randomly assigned in a 1:1 ratio to receive amoxicillin 50 mg/kg per day or placebo oral suspension, in three divided doses orally for 7 days. Patients and investigators were masked to treatment assignment. The primary outcome was the duration of symptoms rated moderately bad or worse (measured using a validated diary) for up to 28 days or until symptoms resolved. The primary outcome and safety were assessed in the intention-to-treat population. The trial is registered with the ISRCTN Registry (ISRCTN79914298).
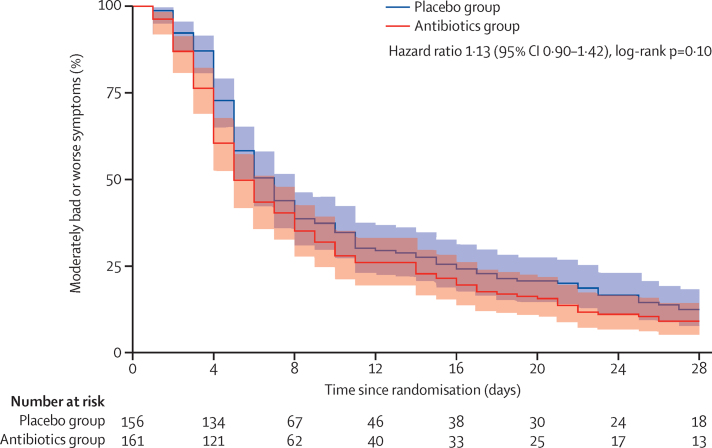
Findings: Between Nov 9, 2016, and March 17, 2020, 432 children (not including six who withdrew permission for use of their data after randomisation) were randomly assigned to the antibiotics group (n=221) or the placebo group (n=211). Complete data for symptom duration were available for 317 (73%) patients; missing data were imputed for the primary analysis. Median durations of moderately bad or worse symptoms were similar between the groups (5 days [IQR 4-11] in the antibiotics group vs 6 days [4-15] in the placebo group; hazard ratio [HR] 1·13 [95% CI 0·90-1·42]). No differences were seen for the primary outcome between the treatment groups in the five prespecified clinical subgroups (patients with chest signs, fever, physician rating of unwell, sputum or chest rattle, and short of breath). Estimates from complete-case analysis and a per-protocol analysis were similar to the imputed data analysis.
Interpretation: Amoxicillin for uncomplicated chest infections in children is unlikely to be clinically effective either overall or for key subgroups in whom antibiotics are commonly prescribed. Unless pneumonia is suspected, clinicians should provide safety-netting advice but not prescribe antibiotics for most children presenting with chest infections.
Funding: National Institute for Health Research.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests SNF is part funded by the Southampton NIHR Biomedical Research Centre. TV reports grants from the EU and the Netherlands Organisation for Health Research and Development, during the conduct of the study; and grants from Abbott, Becton Dickinson, bioMérieux, and Janssen Pharmaceuticals, outside the submitted work. All other authors declare no competing interests.
Figures

Comment in
-
Childhood lower respiratory tract infections: more evidence to do less.Lancet. 2021 Oct 16;398(10309):1383-1384. doi: 10.1016/S0140-6736(21)01955-3. Epub 2021 Sep 22. Lancet. 2021. PMID: 34562390 No abstract available.
References
-
- Davies SC, Fowler T, Watson J, Livermore DM, Walker D. Annual report of the Chief Medical Officer: infection and the rise of antimicrobial resistance. Lancet. 2013;381:1606–1609. - PubMed
-
- Goossens H, Ferech M, Vander Stichele R, Elseviers M. Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet. 2005;365:579–587. - PubMed
-
- Costelloe C, Metcalfe C, Lovering A, Mant D, Hay AD. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. BMJ. 2010;340 - PubMed
-
- Malhotra-Kumar S, Van Heirstraeten L, Coenen S. Impact of amoxicillin therapy on resistance selection in patients with community-acquired lower respiratory tract infections: a randomized, placebo-controlled study. J Antimicrob Chemother. 2016;71:3258–3267. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
