

Evaluating newly approved drugs for multidrug-resistant tuberculosis (endTB): study protocol for an adaptive, multi-country randomized controlled trial
- PMID: 34563240
- PMCID: PMC8465691
- DOI: 10.1186/s13063-021-05491-3
Evaluating newly approved drugs for multidrug-resistant tuberculosis (endTB): study protocol for an adaptive, multi-country randomized controlled trial
Abstract
Background: Treatment of multidrug- and rifampin-resistant tuberculosis (MDR/RR-TB) is expensive, labour-intensive, and associated with substantial adverse events and poor outcomes. While most MDR/RR-TB patients do not receive treatment, many who do are treated for 18 months or more. A shorter all-oral regimen is currently recommended for only a sub-set of MDR/RR-TB. Its use is only conditionally recommended because of very low-quality evidence underpinning the recommendation. Novel combinations of newer and repurposed drugs bring hope in the fight against MDR/RR-TB, but their use has not been optimized in all-oral, shorter regimens. This has greatly limited their impact on the burden of disease. There is, therefore, dire need for high-quality evidence on the performance of new, shortened, injectable-sparing regimens for MDR-TB which can be adapted to individual patients and different settings.
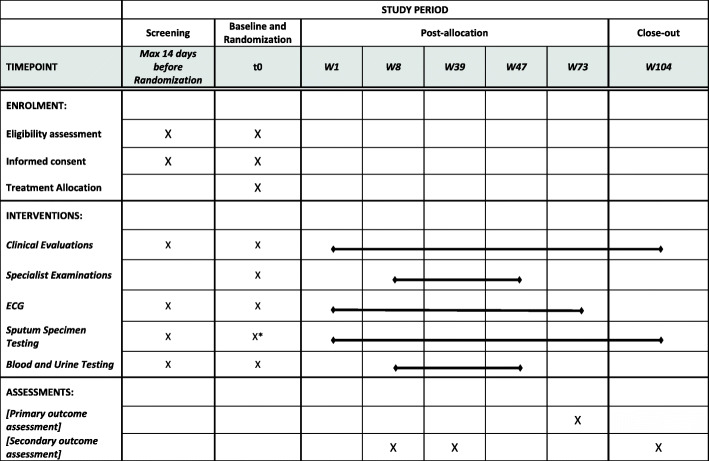
Methods: endTB is a phase III, pragmatic, multi-country, adaptive, randomized, controlled, parallel, open-label clinical trial evaluating the efficacy and safety of shorter treatment regimens containing new drugs for patients with fluoroquinolone-susceptible, rifampin-resistant tuberculosis. Study participants are randomized to either the control arm, based on the current standard of care for MDR/RR-TB, or to one of five 39-week multi-drug regimens containing newly approved and repurposed drugs. Study participation in all arms lasts at least 73 and up to 104 weeks post-randomization. Randomization is response-adapted using interim Bayesian analysis of efficacy endpoints. The primary objective is to assess whether the efficacy of experimental regimens at 73 weeks is non-inferior to that of the control. A sample size of 750 patients across 6 arms affords at least 80% power to detect the non-inferiority of at least 1 (and up to 3) experimental regimens, with a one-sided alpha of 0.025 and a non-inferiority margin of 12%, against the control in both modified intention-to-treat and per protocol populations.
Discussion: The lack of a safe and effective regimen that can be used in all patients is a major obstacle to delivering appropriate treatment to all patients with active MDR/RR-TB. Identifying multiple shorter, safe, and effective regimens has the potential to greatly reduce the burden of this deadly disease worldwide.
Trial registration: ClinicalTrials.gov Identifier NCT02754765. Registered on 28 April 2016; the record was last updated for study protocol version 3.3, on 27 August 2019.
Keywords: Bayesian adaptive randomization; Bedaquiline; Clofazimine; Delamanid; Fluoroquinolone; Linezolid; MDR-TB; Non-inferiority; Pyrazinamide; Rifampicin-resistant tuberculosis; Rifampin-resistant tuberculosis; Treatment shortening.
© 2021. The Author(s).
Conflict of interest statement
The endTB Consortium coordinated donations of delamanid (Otsuka Pharmaceutical) and bedaquiline (Janssen) to be used for treatment by some of the patients included in the endTB Observational Study.
Authors report the following potential conflicts of interest:
None other than the donations disclosed above.
Figures
References
-
- WHO. Global tuberculosis report 2015. Geneva: World Health Organization; 2015.
-
- Siqueira HR, Freitas FA, Oliveira DN, Barreto AM, Dalcolmo MP, Albano RM. Clinical evolution of a group of patients with multidrug-resistant TB treated at a referral center in the city of Rio de Janeiro, Brazil. J Bras Pneumol. 2009. 10.1590/s1806-37132009000100008. - PubMed
-
- Frank M, Adamashvili N, Lomtadze N, Kokhreidze E, Avaliani Z, Kempker RR, Blumberg HM. Long-term Follow-up Reveals High Posttreatment Mortality Rate Among Patients With Extensively Drug-Resistant Tuberculosis in the Country of Georgia. Open Forum Infect Dis. 2019. 10.1093/ofid/ofz152. - PMC - PubMed
-
- WHO. WHO consolidated guidelines on tuberculosis. Module 4: treatment - drug-resistant tuberculosis treatment. Geneva: World Health Organization; 2020. - PubMed
-
- Bonnet M, Bastard M, du Cros P, Khamraev A, Kimenye K, Khurkhumal S, et al. Identification of patients who could benefit from bedaquiline or delamanid: a multisite MDR-TB cohort study. Int J Tuberc Lung Dis. 2016. 10.5588/ijtld.15.0962. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
