

Racial and ethnic differences in perception of provider cultural competence among patients with depression and anxiety symptoms: a retrospective, population-based, cross-sectional analysis
- PMID: 34563316
- PMCID: PMC10688309
- DOI: 10.1016/S2215-0366(21)00285-6
Racial and ethnic differences in perception of provider cultural competence among patients with depression and anxiety symptoms: a retrospective, population-based, cross-sectional analysis
Abstract
Background: Racial and ethnic minorities face disparities in access to health care. Culturally competent care might lessen these disparities. Few studies have studied the patients' view of providers' cultural competence, especially in psychiatric care. We aimed to examine the associations of race, ethnicity, and mental health status with patient-reported importance of provider cultural competence.
Methods: Our retrospective, population-based, cross-sectional study used data extracted from self-reported questionnaires of adults aged at least 18 years who participated in the US National Health Interview Survey (NHIS; 2017 cycle). We included data on all respondents who answered supplementary cultural competence questions and the Adult Functioning and Disability survey within the NHIS. We classified participants as having anxiety or depression if they reported symptoms at least once a week or more often, and responded that the last time they had symptoms the intensity was "somewhere between a little and a lot" or "a lot." Participant answers to cultural competency survey questions (participant desire for providers to understand or share their culture, and frequency of access to providers who share their culture) were the outcome variables. Multivariable ordinal logistic regressions were used to estimate adjusted odds ratios (aORs) for the outcome variables in relation to sociodemographic characteristics (including race and ethnicity), self-reported health status, and presence of symptoms of depression, anxiety, or both.
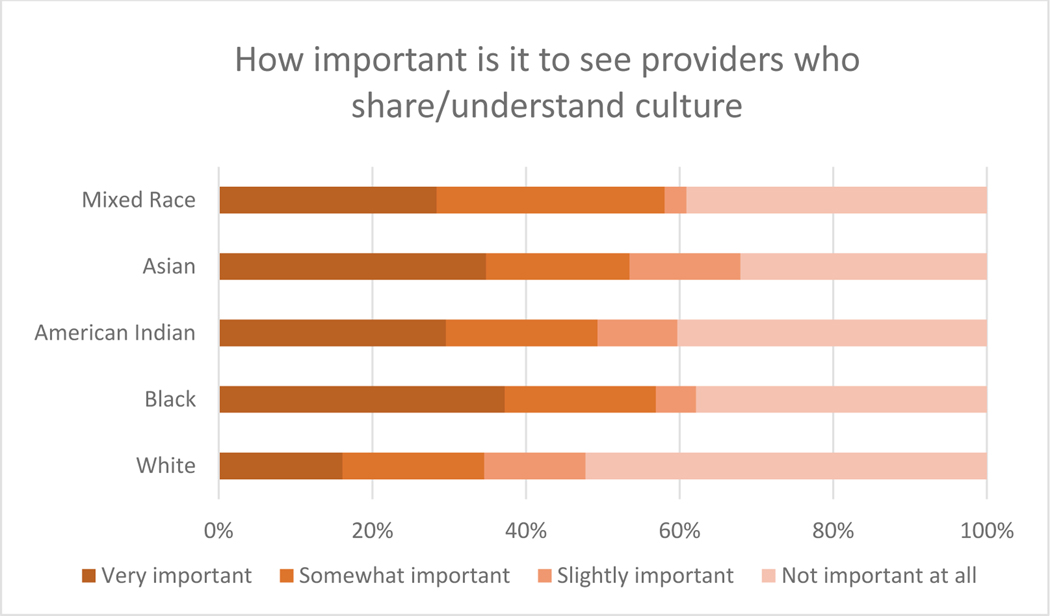
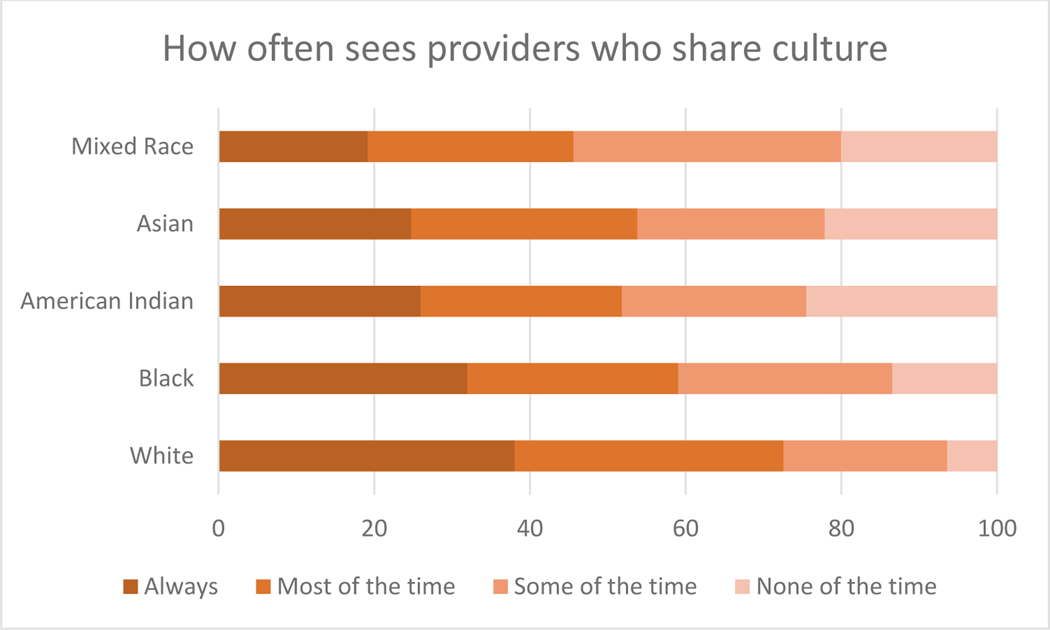
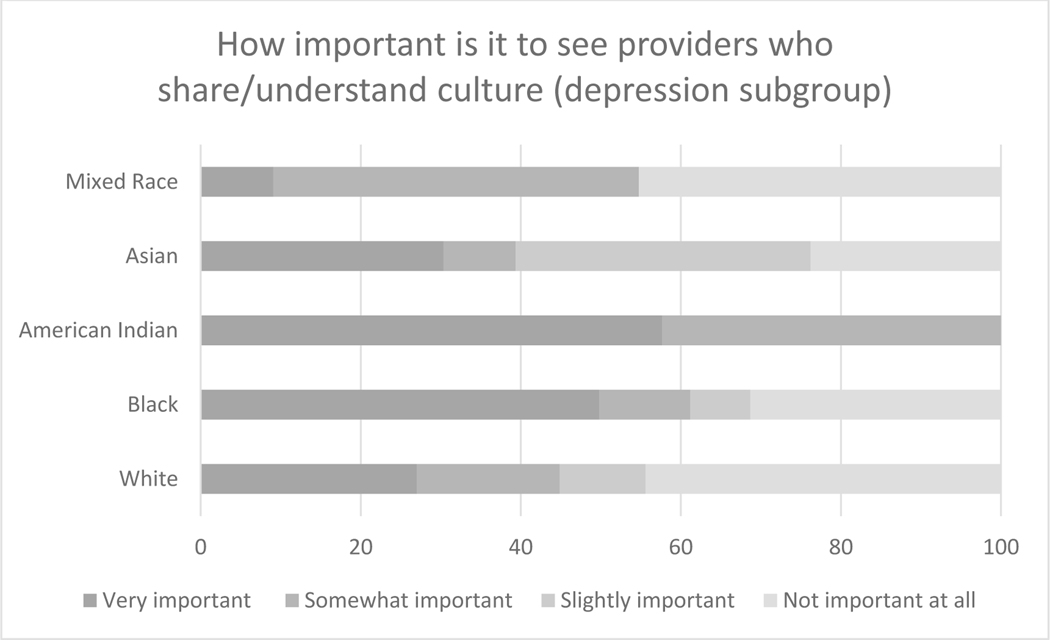
Findings: 3910 people had available data for analysis. Mean age was 52 years (IQR 36-64). 1422 (39·2%, sample weight adjusted) of the participants were men and 2488 (60·9%) were women. 3290 (82·7%) were White, 346 (9·1%) were Black or African American, 31 (0·8%) were American Indian or Alaskan Native, 144 (4·8%) were Asian American, and 99 (2·6%) were Mixed Race. 380 (12·5%) identified as Hispanic ethnicity and 3530 (87·5%) as non-Hispanic. Groups who were more likely to express a desire for their providers to share or understand their culture included participants who had depression symptoms (vs those without depression or anxiety symptoms, aOR 1·57 [95% CI 1·13-2·19], p=0·008) and participants who were of a racial minority group (Black vs White, aOR 2·54 [1·86-3·48], p=0·008; Asian American vs White, aOR 2·57 [1·66-3·99], p<0·001; and Mixed Race vs White, aOR 1·69 [1·01-2·82], p=0·045) or ethnic minority group (Hispanic vs non-Hispanic, aOR 2·69 [2·02-3·60], p<0·001); these groups were less likely to report frequently being able to see providers who shared their culture (patients with depression symptoms vs those without depression or anxiety symptoms, aOR 0·63 (0·41-0·96); p=0·030; Black vs White, aOR 0·56 [0·38-0·84], p=0·005; Asian American vs White, aOR 0·38 [0·20-0·72], p=0·003; Mixed Race vs White, aOR 0·35 [0·19-0·64], p=0·001; Hispanic vs non-Hispanic, aOR 0·61 [0·42-0·89], p=0·010). On subgroup analysis of participants reporting depression symptoms, patients who identified their race as Black or African American, or American Indian or Alaskan Native, and those who identified as Hispanic ethnicity, were more likely to report a desire for provider cultural competence.
Interpretation: Racial and ethnic disparities exist in how patients perceive their providers' cultural competence, and disparities are pronounced in patients with depression. Developing a culturally competent and humble approach to care is crucial for mental health providers.
Funding: None.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
Similar articles
-
Disparities by Race/Ethnicity and Immigration Status in Perceived Importance of and Access to Culturally Competent Health Care in the United States.J Racial Ethn Health Disparities. 2024 Jun;11(3):1829-1841. doi: 10.1007/s40615-023-01655-w. Epub 2023 Jun 14. J Racial Ethn Health Disparities. 2024. PMID: 37314687
-
Racial/Ethnic Disparities in the Performance of Prediction Models for Death by Suicide After Mental Health Visits.JAMA Psychiatry. 2021 Jul 1;78(7):726-734. doi: 10.1001/jamapsychiatry.2021.0493. JAMA Psychiatry. 2021. PMID: 33909019 Free PMC article.
-
Racial and Ethnic Disparities in Diabetes Screening Between Asian Americans and Other Adults: BRFSS 2012-2014.J Gen Intern Med. 2017 Apr;32(4):423-429. doi: 10.1007/s11606-016-3913-x. Epub 2016 Nov 15. J Gen Intern Med. 2017. PMID: 27848187 Free PMC article.
-
Comparing Preferences for Depression and Diabetes Treatment among Adults of Different Racial and Ethnic Groups Who Reported Discrimination in Health Care [Internet].Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2021 Jan. Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2021 Jan. PMID: 38478703 Free Books & Documents. Review.
-
Improving Cultural Competence to Reduce Health Disparities [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2016 Mar. Report No.: 16-EHC006-EF. Rockville (MD): Agency for Healthcare Research and Quality (US); 2016 Mar. Report No.: 16-EHC006-EF. PMID: 27148614 Free Books & Documents. Review.
Cited by
-
Testing the Assumptions in the Process of Cultural Competence in the Delivery of Healthcare Services Using Empirical Data, Focusing on Cultural Awareness.J Transcult Nurs. 2023 May;34(3):187-194. doi: 10.1177/10436596231152212. Epub 2023 Feb 9. J Transcult Nurs. 2023. PMID: 36759971 Free PMC article.
-
Enhancing cultural sensitivity in medical education: a central pillar for patient-centered care.Korean J Med Educ. 2025 Jun;37(2):225-229. doi: 10.3946/kjme.2025.337. Epub 2025 May 29. Korean J Med Educ. 2025. PMID: 40468498 Free PMC article. No abstract available.
-
Providers' perspectives on the impact of culture in the recognition and diagnosis of anxiety.J Mood Anxiety Disord. 2023 Sep 29;4:100030. doi: 10.1016/j.xjmad.2023.100030. eCollection 2023 Dec. J Mood Anxiety Disord. 2023. PMID: 40656970 Free PMC article.
-
Depression as a Mediator and Social Participation as a Moderator in the Bidirectional Relationship Between Sleep Disorders and Pain: Dynamic Cohort Study.JMIR Public Health Surveill. 2023 Jul 26;9:e48032. doi: 10.2196/48032. JMIR Public Health Surveill. 2023. PMID: 37494109 Free PMC article.
-
Disparities by Race/Ethnicity and Immigration Status in Perceived Importance of and Access to Culturally Competent Health Care in the United States.J Racial Ethn Health Disparities. 2024 Jun;11(3):1829-1841. doi: 10.1007/s40615-023-01655-w. Epub 2023 Jun 14. J Racial Ethn Health Disparities. 2024. PMID: 37314687
References
-
- Qureshi A, Collazos F, Ramos M, et al. What is the key to culturally competent care: Reducing bias or cultural tailoring? HHS Public Access Author manuscript. Health Aff. 2005;2(4):810–818. doi:10.1080/08870446.2017.1284221 - DOI
-
- Blanco C, Patel SR, Liu L, Jiang H, Lewis-Fernández R, Schmidt AB, ... & Olfson M. National trends in ethnic disparities in mental health care. Med Care. 2007:1012–1019. - PubMed
