

Comparative performance of risk prediction models for hepatitis B-related hepatocellular carcinoma in the United States
- PMID: 34563579
- PMCID: PMC8786210
- DOI: 10.1016/j.jhep.2021.09.009
Comparative performance of risk prediction models for hepatitis B-related hepatocellular carcinoma in the United States
Abstract
Background & aims: Guidelines recommend hepatocellular carcinoma (HCC) surveillance in patients with chronic HBV infection. Several HCC risk prediction models are available to guide surveillance decisions, but their comparative performance remains unclear.
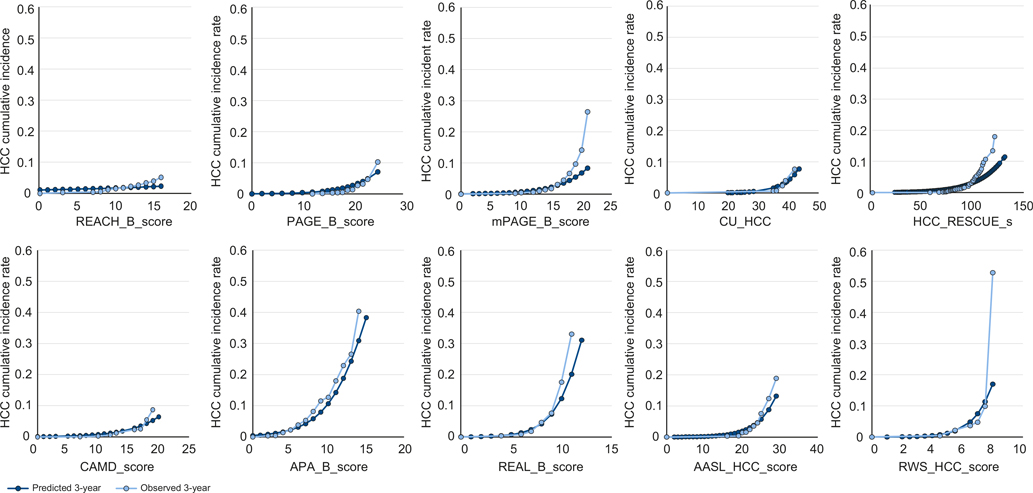
Methods: Using a retrospective cohort of patients with HBV treated with nucleos(t)ide analogues at 130 Veterans Administration facilities between 9/1/2008 and 12/31/2018, we calculated risk scores from 10 HCC risk prediction models (REACH-B, PAGE-B, m-PAGE-B, CU-HCC, HCC-RESCUE, CAMD, APA-B, REAL-B, AASL-HCC, RWS-HCC). We estimated the models' discrimination and calibration. We calculated HCC incidence in risk categories defined by the reported cut-offs for all models.
Results: Of 3,101 patients with HBV (32.2% with cirrhosis), 47.0% were treated with entecavir, 40.6% tenofovir, and 12.4% received both. During a median follow-up of 4.5 years, 113 patients developed HCC at an incidence of 0.75/100 person-years. AUC values for 3-year HCC risk were the highest for RWS-HCC, APA-B, REAL-B, and AASL-HCC (all >0.80). Of these, 3 (APA-B, RWS-HCC, REAL-B) incorporated alpha-fetoprotein. AUC values for the other models ranged from 0.73 for PAGE-B to 0.79 for CAMD and HCC-RESCUE. Of the 7 models with AUC >0.75, only APA-B was poorly calibrated. In total, 10-20% of the cohort was deemed low-risk based on the published cut-offs. None of the patients in the low-risk groups defined by PAGE-B, m-PAGE-B, AASL-HCC, and REAL-B developed HCC during the study timeframe.
Conclusion: In this national cohort of US-based patients with HBV on antiviral treatment, most models performed well in predicting HCC risk. A low-risk group, in which no cases of HCC occurred within a 3-year timeframe, was identified by several models (PAGE-B, m-PAGE-B, CAMD, AASL-HCC, REAL-B). Further studies are warranted to examine whether these patients could be excluded from HCC surveillance.
Lay summary: Risk prediction models for hepatocellular carcinoma (HCC) in patients infected with hepatitis B virus (HBV) could guide HCC surveillance decisions. In this large cohort of US-based patients receiving treatment for HBV, most published models discriminated between those who did or did not develop HCC, although the RWS-HCC, REAL-B, and AASL-HCC performed the best. If confirmed in future studies, these models could help identify a low-risk subset of patients on antiviral treatment who could be excluded from HCC surveillance.
Keywords: Hepatitis B virus; external validation; hepatocelluar carcinoma.
Copyright © 2021. Published by Elsevier B.V.
Conflict of interest statement
Conflict of interest The authors declare no conflicts of interest that pertain to this work. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures
Comment in
-
Which risk model can better predict hepatocellular carcinoma in hepatitis B patients with an antiviral treatment duration of over 1 year?J Hepatol. 2024 Apr;80(4):e160. doi: 10.1016/j.jhep.2023.06.014. Epub 2023 Jul 4. J Hepatol. 2024. PMID: 37414258 No abstract available.
References
-
- Polaris Observatory C. Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: a modelling study. Lancet Gastroenterol Hepatol 2018;3:383–403. - PubMed
-
- Kim WR. Risk of incident hepatocellular carcinoma in hepatitis B-infected patients treated with tenofovir disoproxil fumarate versus entecavir: a US administrative claims analysis. Hepatology 2019;70:302A–303A.
-
- Yang HI, Yuen MF, Chan HL, Han KH, Chen PJ, Kim DY, et al. Risk estimation for hepatocellular carcinoma in chronic hepatitis B (REACH-B): development and validation of a predictive score. Lancet Oncol 2011;12:568–574. - PubMed
-
- Papatheodoridis G, Dalekos G, Sypsa V, Yurdaydin C, Buti M, Goulis J, et al. PAGE-B predicts the risk of developing hepatocellular carcinoma in Caucasians with chronic hepatitis B on 5-year antiviral therapy. J Hepatol 2016;64:800–806. - PubMed
-
- Kim JH, Kim YD, Lee M, Jun BG, Kim TS, Suk KT, et al. Modified PAGE-B score predicts the risk of hepatocellular carcinoma in Asians with chronic hepatitis B on antiviral therapy. J Hepatol 2018;69:1066–1073. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
