

Clinical efficacy and safety evaluation of favipiravir in treating patients with severe fever with thrombocytopenia syndrome
- PMID: 34563924
- PMCID: PMC8479638
- DOI: 10.1016/j.ebiom.2021.103591
Clinical efficacy and safety evaluation of favipiravir in treating patients with severe fever with thrombocytopenia syndrome
Abstract
Background: Severe fever with thrombocytopenia syndrome (SFTS) is an emerging infectious disease with high mortality, however with no effective therapy available.
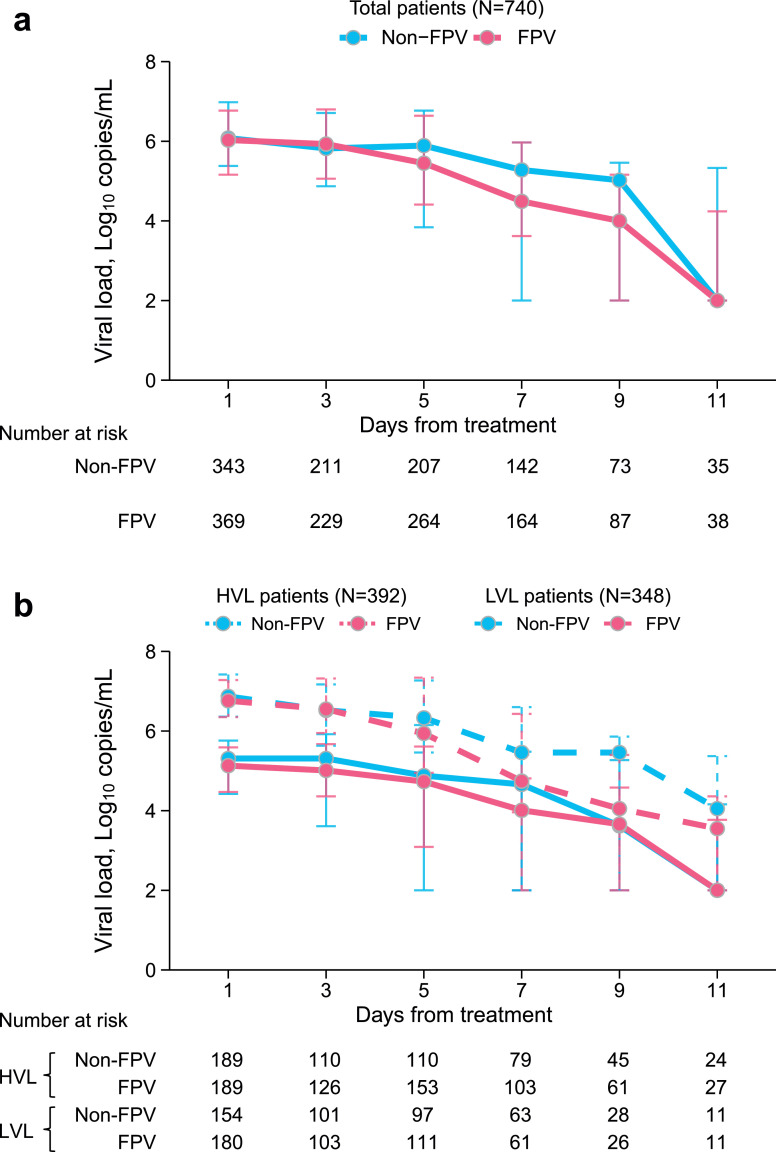
Methods: The effect of favipiravir (FPV) in treating SFTS was evaluated by an integrated analysis on data collected from a single-arm study (n=428), a surveillance study (n=2350) and published data from a randomized controlled trial study (n=145). A 1:1 propensity score matching was performed to include 780 patients: 390 received FPV and 390 received supportive therapy only. Case fatality rates (CFRs), clinical progress, and adverse effects were compared.
Findings: FPV treatment had significantly reduced CFR from 20.0% to 9.0% (odds ratio 0.38, 95% confidence interval 0.23-0.65), however showing heterogeneity when patients were grouped by age, onset-to-admission interval, initial viral load and therapy duration. The effect of FPV was significant only among patients aged ≤70 years, with onset-to-admission interval ≤5 days, therapy duration ≥5 days or baseline viral load ≤1 × 106 copies/mL. Age-stratified analysis revealed no benefit in the aging group >70 years, regardless of their sex, onset-to-admission interval, therapy duration or baseline viral load. However, for both ≤60 and 60-70 years groups, therapy duration and baseline viral load differentially affected FPV therapy efficiency. Hyperuricemia and thrombocytopenia, as the major adverse response of FPV usage, were observed in >70 years patients.
Interpretation: FPV was safe in treating SFTS patients but showed no benefit for those aged >70 years. Instant FPV therapy could highly benefit SFTS patients aged 60-70 years.
Funding: China Natural Science Foundation (No. 81825019, 82073617 and 81722041) and China Mega-project for Infectious Diseases (2018ZX10713002 and 2015ZX09102022).
Keywords: Efficacy; Favipiravir; Heterogeneity; Safety; Severe fever with thrombocytopenia syndrome.
Copyright © 2021 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that no conflict of interest exists.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
