

10-Year Clinical, Functional, and X-ray Follow-Up Evaluation of a Novel Posterior Percutaneous Screw-Rod Instrumentation Technique for Single-Level Pyogenic Spondylodiscitis
- PMID: 34564543
- PMCID: PMC8482233
- DOI: 10.3390/tropicalmed6030159
10-Year Clinical, Functional, and X-ray Follow-Up Evaluation of a Novel Posterior Percutaneous Screw-Rod Instrumentation Technique for Single-Level Pyogenic Spondylodiscitis
Abstract
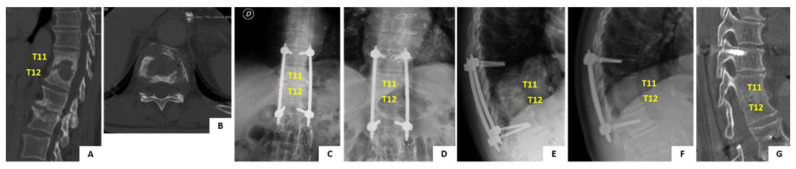
Medical treatment with antibiotic therapy remains the mainstay of treatment for pyogenic spondylodiscitis (PS). Nevertheless, orthopaedic treatment is also very important in relieving pain, preventing neurological damage, and avoiding development of spinal deformities (e.g., scoliosis, kyphosis) due to spinal instability. Rigid thoracolumbosacral orthosis (TLSO) bracing is often needed in patients with PS, and average duration of treatment of 3 to 4 months. However, TLSO bracing can be poorly tolerated and limit ability of the patient to go back to a normal life. In 2004 our group developed an alternative surgical treatment to TLSO bracing by percutaneous posterior screw-rod bridge instrumentation of the infected level. This treatment allows early and free mobilization of the patients and is associated with faster recovery, lower pain scores and improved quality of life as previously reported. Herein, we report the clinical outcome of the first 3 patients who have completed the 10 years follow-up mark after the procedure. A case report is also described and details of the procedure are provided.
Keywords: minimally-invasive spinal surgery; percutaneous posterior spinal stabilization; pyogenic spondylodiscitis; spinal infections; surgical treatment of pyogenic spondylodiscitis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




Similar articles
-
Is posterior percutaneous screw-rod instrumentation a safe and effective alternative approach to TLSO rigid bracing for single-level pyogenic spondylodiscitis? Results of a retrospective cohort analysis.Spine J. 2014 Jul 1;14(7):1139-46. doi: 10.1016/j.spinee.2013.07.479. Epub 2013 Oct 16. Spine J. 2014. PMID: 24139231
-
Comparison of two-stage open versus percutaneous pedicle screw fixation in treating pyogenic spondylodiscitis.BMC Musculoskelet Disord. 2014 Dec 18;15:443. doi: 10.1186/1471-2474-15-443. BMC Musculoskelet Disord. 2014. PMID: 25519761 Free PMC article.
-
Surgical results of long posterior fixation with short fusion in the treatment of pyogenic spondylodiscitis of the thoracic and lumbar spine: a retrospective study.Spine (Phila Pa 1976). 2012 Dec 1;37(25):E1572-9. doi: 10.1097/BRS.0b013e31827399b8. Spine (Phila Pa 1976). 2012. PMID: 22996263
-
Posterior Vertebral Column Resection for Severe and Rigid Spinal Deformity Associated With Neurological Deficit After Implant Removal Following Posterior Instrumented Fusion: A Case Report and Literature Review.Spine (Phila Pa 1976). 2015 Jul 1;40(13):E794-8. doi: 10.1097/BRS.0000000000000921. Spine (Phila Pa 1976). 2015. PMID: 25893358 Review.
-
The Need for Comprehensive Medical Management in Pyogenic Spondylodiscitis: A Review Article.Spine Surg Relat Res. 2023 Nov 2;8(3):243-252. doi: 10.22603/ssrr.2023-0155. eCollection 2024 May 27. Spine Surg Relat Res. 2023. PMID: 38868783 Free PMC article. Review.
Cited by
-
What Is Worse: A Comparison of Solitary Versus Multifocal Pyogenic Spondylodiscitis Using a Nationwide Analysis of Readmission Rates and Risk Factors.J Clin Med. 2025 Aug 15;14(16):5784. doi: 10.3390/jcm14165784. J Clin Med. 2025. PMID: 40869609 Free PMC article.
References
-
- Fantoni M., Trecarichi E.M., Rossi B., Mazzotta V., Di Giacomo G., Nasto L.A., Di Meco E., Pola E. Epidemiological and clinical features of pyogenic spondylodiscitis. Eur. Rev. Med. Pharmacol. Sci. 2012;16:2–7. - PubMed
-
- Pola E., Taccari F., Autore G., Giovannenze F., Pambianco V., Cauda R., Maccauro G., Fantoni M. Multidisciplinary management of pyogenic spondylodiscitis: Epidemiological and clinical features, prognostic factors and long-term outcomes in 207 patients. Eur. Spine J. 2018;27:229–236. doi: 10.1007/s00586-018-5598-9. - DOI - PubMed
-
- Berbari E.F., Kanj S.S., Kowalski T.J., Darouiche R.O., Widmer A.F., Schmitt S.K., Hendershot E.F., Holtom P.D., Huddleston P.M., Petermann G.W., et al. 2015 Infectious Diseases Society of America (IDSA) Clinical Practice Guidelines for the Diagnosis and Treatment of Native Vertebral Osteomyelitis in Adults. Clin. Infect. Dis. 2015;61:e26–e46. doi: 10.1093/cid/civ482. - DOI - PubMed
LinkOut - more resources
Full Text Sources
