

Use of Intravaginal Progesterone-Releasing Device Results in Similar Pregnancy Rates and Losses to Long-Acting Progesterone to Synchronize Acyclic Embryo Recipient Mares
- PMID: 34564584
- PMCID: PMC8472191
- DOI: 10.3390/vetsci8090190
Use of Intravaginal Progesterone-Releasing Device Results in Similar Pregnancy Rates and Losses to Long-Acting Progesterone to Synchronize Acyclic Embryo Recipient Mares
Abstract
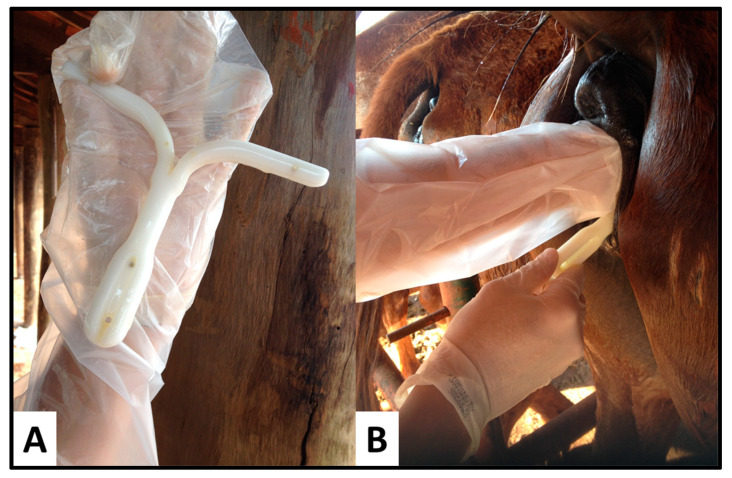
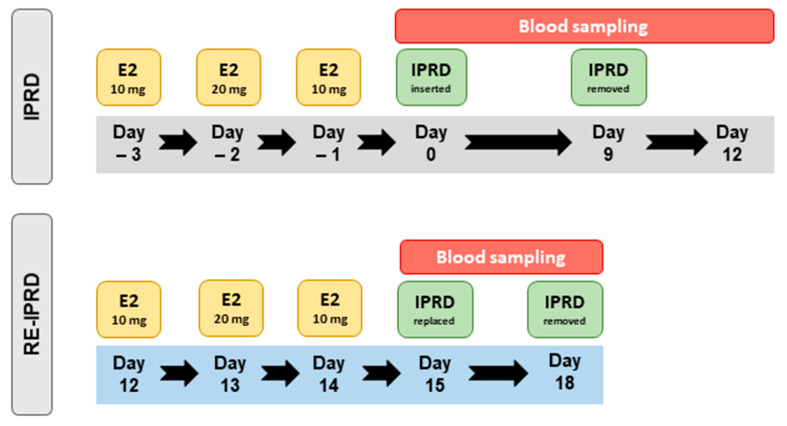
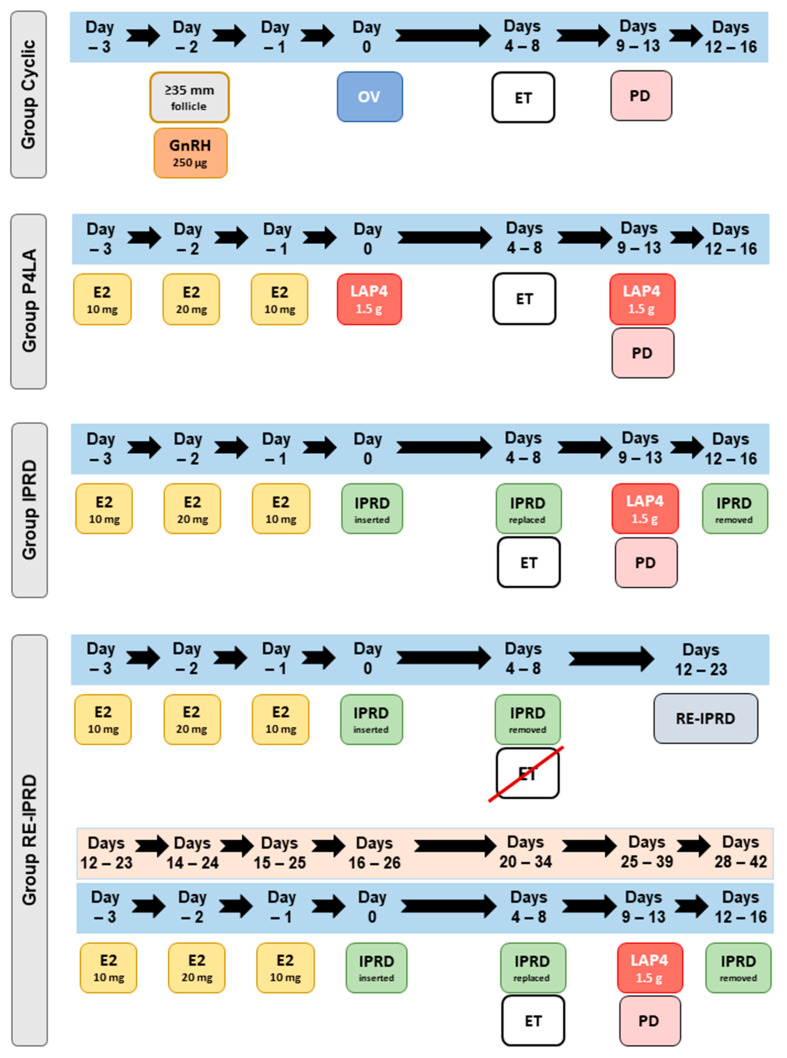
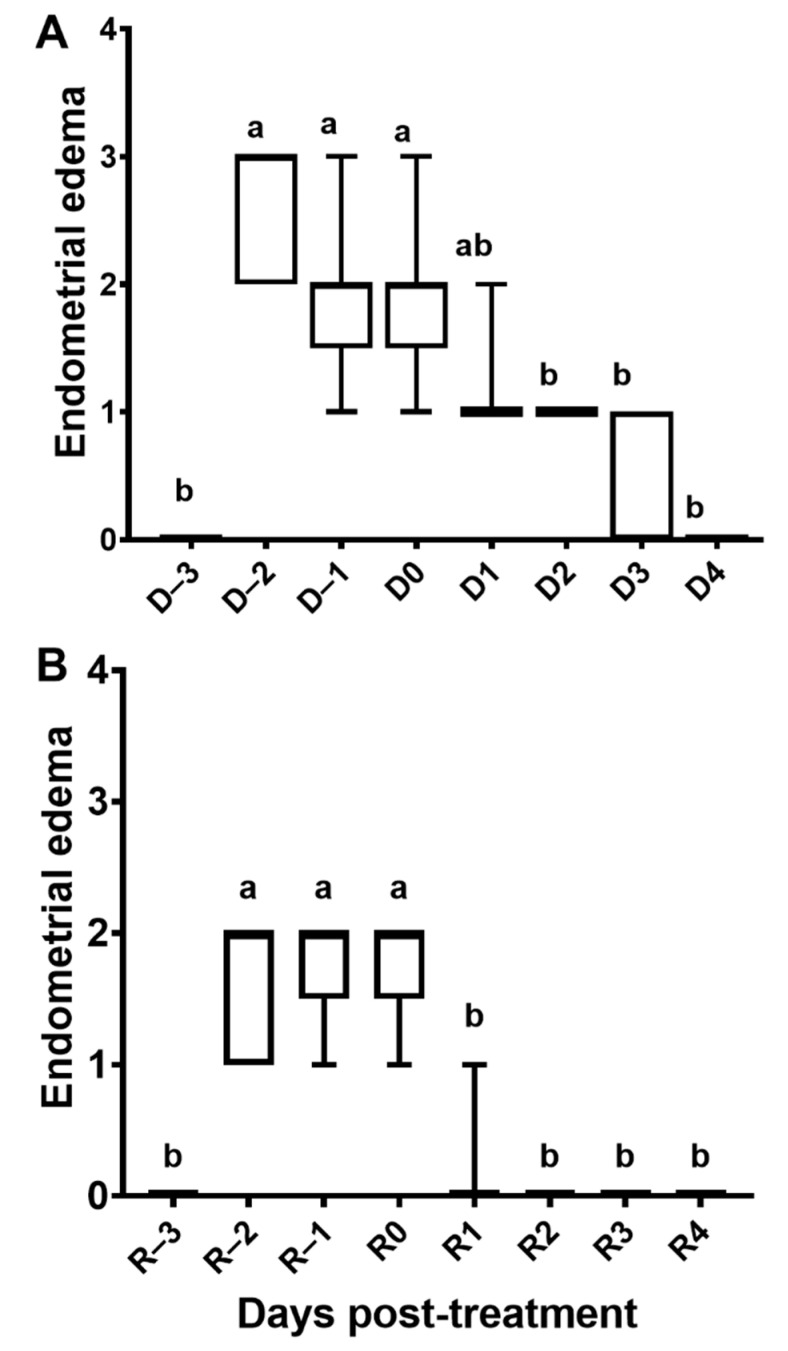
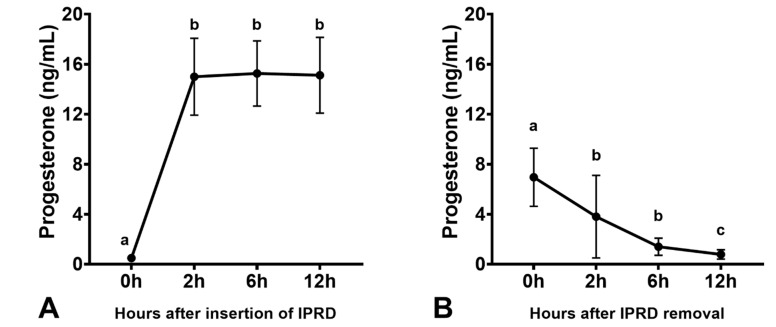
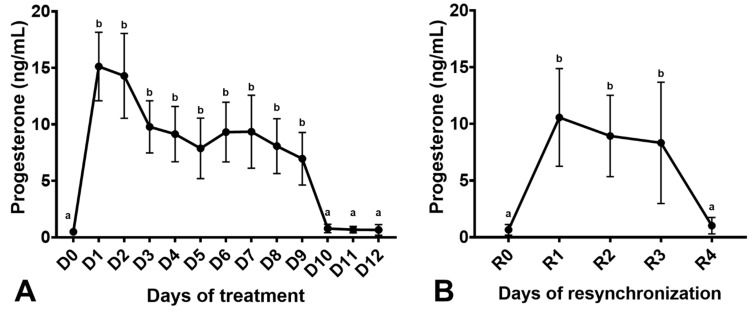
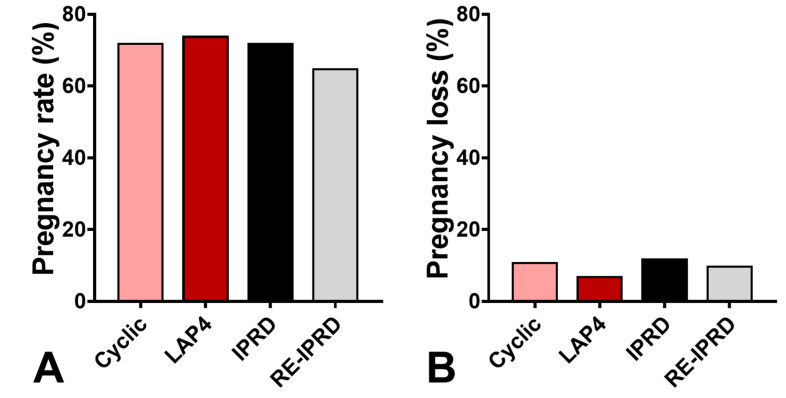
The objectives of this study were: (1) to assess uterine features and serum progesterone concentrations of acyclic mares synchronized and resynchronized with intravaginal progesterone release device (IPRD), and (2) to compare pregnancy rates and losses of cyclic and acyclic embryo recipient mares treated with different synchronization protocols. In Experiment 1, mares (n = 12) received estradiol for 3 days (E2-3d), and then 24 h after the last injection, an IPRD was inserted and kept in place for 9 days. Three days after IPRD removal, mares were treated with E2-3d, and then a new IPRD was inserted and maintained for three days. Serum progesterone concentrations were assessed 2, 6, and 12 h after insertion and removal of IPRD, and then daily from the insertion of the first IPRD to one day after removal of the second IPRD. Experiment 2 was conducted with embryo recipient mares randomly assigned to four groups: (1) Cyclic: mares (n = 75) had ovulation confirmed after receiving a single dose of histrelin when a periovulatory follicle was first detected, (2) LAP4: acyclic mares (n = 92) were treated with E2-3d and then administered a single dose of LAP4 24 h after the last estradiol injection, (3) IPRD: acyclic mares (n = 130) were treated with E2-3d and an IPRD for 4-8 days, and (4) RE-IPRD: acyclic mares (n = 32) were synchronized as in the IPRD group but not used for embryo transfer (ET), then 8 to 15 days later, the mares were resynchronized with E2-3d and an IPRD for 4-8 days. In vivo-produced Day-8 embryos were collected and transferred 4-8 days after ovulation or progesterone treatments. Mares in IPRD and RE-IPRD groups had the intravaginal device removed immediately before ET, and then a new IPRD was inserted right after ET. Pregnancy diagnosis was performed at 5, 30, and 60 days after ET. Once pregnancy was confirmed, mares in the three acyclic groups received weekly injections of LAP4 (1.5 g) until 120 days of pregnancy. Mares in IPRD and RE-IPRD groups had the device removed three days after the first pregnancy diagnosis. In Experiment 1, progesterone concentrations increased rapidly starting 2 h after insertion of IPRD (p < 0.05); then, concentrations plateaued well above pregnancy maintenance until removal on days 9 and 3, respectively. Progesterone concentrations were reduced to baseline 24 h after IPRD removal (p < 0.05). For experiment 2, there was no difference in pregnancy rates across groups (65-74%) or pregnancy losses by 60 days of gestation (7-12%) (p > 0.05). In conclusion, the IPRD used herein resulted in a rapid increase and a sharp decline in progesterone concentrations upon its insertion and removal, respectively. Finally, our results demonstrated that IPRD could be a compatible alternative to LAP4 to synchronize and resynchronize acyclic embryo recipient mares.
Keywords: embryo transfer; equine; fertility; hormonal therapy; recipient mare.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Serum Progesterone and Conception Rates in Acyclic Embryo Recipient Mares Using a Bovine Progesterone-Releasing Intravaginal Device.J Equine Vet Sci. 2021 Feb;97:103325. doi: 10.1016/j.jevs.2020.103325. Epub 2020 Nov 21. J Equine Vet Sci. 2021. PMID: 33478762
-
Synchronization of cyclic and acyclic embryo recipient mares with donor mares.Anim Reprod Sci. 2018 Mar;190:1-9. doi: 10.1016/j.anireprosci.2017.12.016. Epub 2017 Dec 23. Anim Reprod Sci. 2018. PMID: 29373173
-
Animal-level factors affecting ovarian function in Bos indicus heifers treated to synchronize ovulation with intravaginal progesterone-releasing devices and oestradiol benzoate.Reprod Domest Anim. 2012 Jun;47(3):463-71. doi: 10.1111/j.1439-0531.2011.01905.x. Epub 2011 Oct 3. Reprod Domest Anim. 2012. PMID: 22497623
-
Ovarian responses in Bos indicus heifers treated to synchronise ovulation with intravaginal progesterone releasing devices, oestradiol benzoate, prostaglandin F(2α) and equine chorionic gonadotrophin.Anim Reprod Sci. 2011 Dec;129(3-4):118-26. doi: 10.1016/j.anireprosci.2011.11.001. Epub 2011 Nov 15. Anim Reprod Sci. 2011. PMID: 22136725
-
Ovulation, pregnancy rate and early embryonic development in vernal transitional mares treated with equine- or porcine-FSH.Reprod Domest Anim. 2010 Apr;45(2):287-94. doi: 10.1111/j.1439-0531.2008.01296.x. Epub 2009 Jan 8. Reprod Domest Anim. 2010. PMID: 19144034 Review.
Cited by
-
Assisted Reproductive Technologies (ARTs) in Domestic Mammals.Vet Sci. 2023 Apr 11;10(4):287. doi: 10.3390/vetsci10040287. Vet Sci. 2023. PMID: 37104442 Free PMC article.
References
-
- McCue P., Squires E. Equine Embryo Transfer. 1st ed. CRC Press; Boca Raton, FL, USA: 2015.
-
- Allen W.R., Rowson L.E. Surgical and non-surgical egg transfer in horses. J. Reprod. Fertil. Suppl. 1975;23:525–530. - PubMed
LinkOut - more resources
Full Text Sources
