

Racial Differences in Prevalence and Treatment for Psoriatic Arthritis and Ankylosing Spondylitis by Insurance Coverage in the USA
- PMID: 34564835
- PMCID: PMC8475338
- DOI: 10.1007/s40744-021-00370-4
Racial Differences in Prevalence and Treatment for Psoriatic Arthritis and Ankylosing Spondylitis by Insurance Coverage in the USA
Abstract
Introduction: Patients with psoriatic arthritis (PsA) and ankylosing spondylitis (AS) may receive suboptimal care, and differences in care by race/ethnicity, sex, and insurance coverage are not well studied.
Methods: This was a descriptive, retrospective cross-sectional US claims database analysis utilizing the Medicaid multi-state segment of the IBM® MarketScan® Commercial Claims and Encounters Supplemental Database and Optum Insight Clinformatics® Data Mart database for 2019. Patients aged ≥ 18 years with PsA or AS and continuous medical and pharmacy coverage were included. Outcomes evaluated were prevalence and percentage of patients receiving biologic disease-modifying antirheumatic drugs (bDMARDs)/targeted synthetic DMARDs (tsDMARDs) or visiting a rheumatologist. Outcomes were stratified by race/ethnicity, sex, and insurance coverage, with outcomes determined for commercial insurance, Medicare, and Medicaid enrollees. Differences observed in outcomes were numerical in nature.
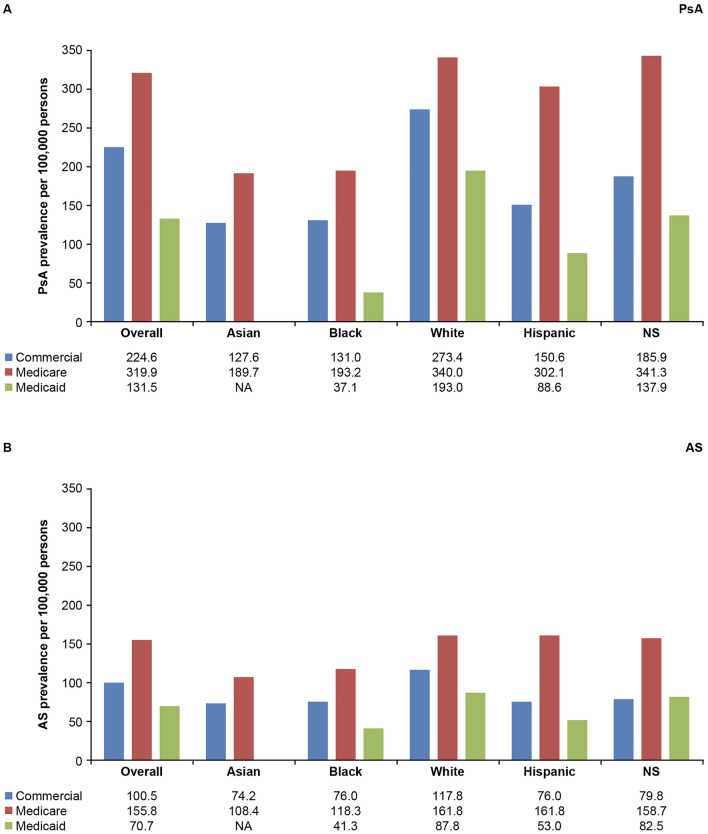
Results: Prevalences of PsA and AS were highest for Medicare enrollees (320 and 156 per 100,000 persons [0.32 and 0.16%], respectively) and lowest for Medicaid enrollees (132 and 71 per 100,000 persons [0.13 and 0.07%], respectively). White patients had the greatest prevalence versus patients of other races/ethnicities. Females had a higher prevalence of PsA than males, while AS prevalence was generally lower for females versus males for each insurance category. The percentage of patients prescribed bDMARDs/tsDMARDs was highest for commercial insurance enrollees (PsA 63%, AS 43%) and lowest for Medicare enrollees (PsA 21%, AS 11%). The proportion of patients who saw a rheumatologist was lower for Medicaid enrollees (PsA 12%, AS 10%) than for commercial insurance or Medicare enrollees (PsA 68%, 55%; AS 67%, 42%). For commercial insurance and Medicare enrollees, the percentage of patients visiting a rheumatologist was similar by race/ethnicity but higher for females versus males.
Conclusions: The prevalence and treatment of PsA and AS differs by race/ethnicity, insurance coverage, and sex in the USA. Efforts for improving access to care are needed to improve outcomes among all patients.
Keywords: Ankylosing spondylitis; Commercial insurance; Medicaid; Medicare; Prevalence; Psoriatic arthritis; Rheumatologist; Targeted immunomodulator; USA.
© 2021. The Author(s).
Figures


References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
