

Transcranial direct current stimulation combined with robotic therapy for upper and lower limb function after stroke: a systematic review and meta-analysis of randomized control trials
- PMID: 34565399
- PMCID: PMC8474736
- DOI: 10.1186/s12984-021-00941-0
Transcranial direct current stimulation combined with robotic therapy for upper and lower limb function after stroke: a systematic review and meta-analysis of randomized control trials
Abstract
Background: Transcranial direct current stimulation (tDCS) is a non-invasive brain stimulation method able to modulate neuronal activity after stroke. The aim of this systematic review was to determine if tDCS combined with robotic therapy (RT) improves limb function after stroke when compared to RT alone.
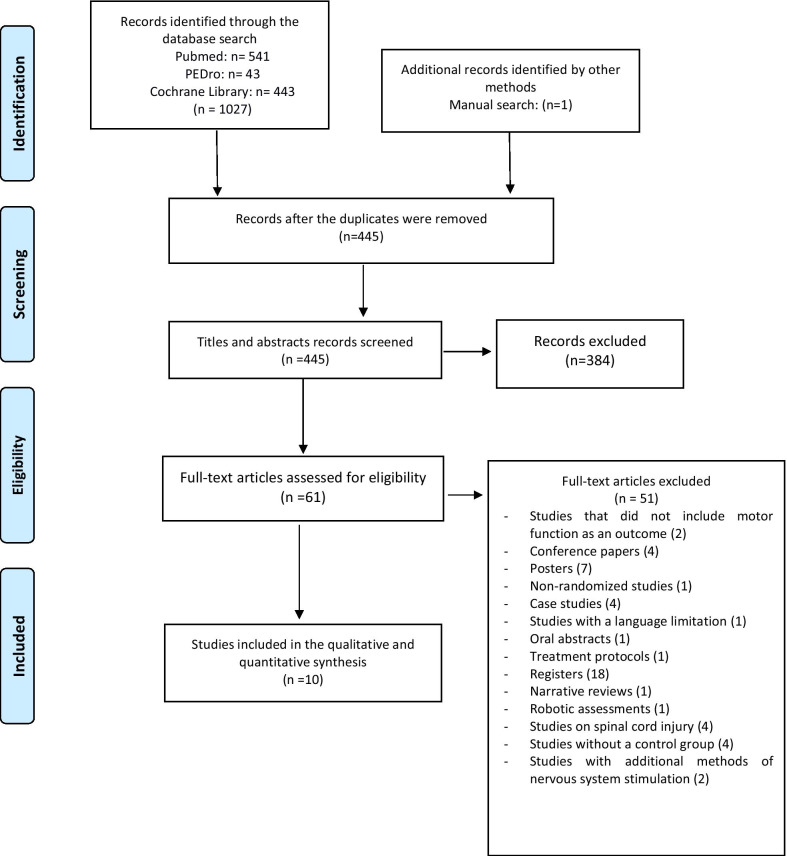
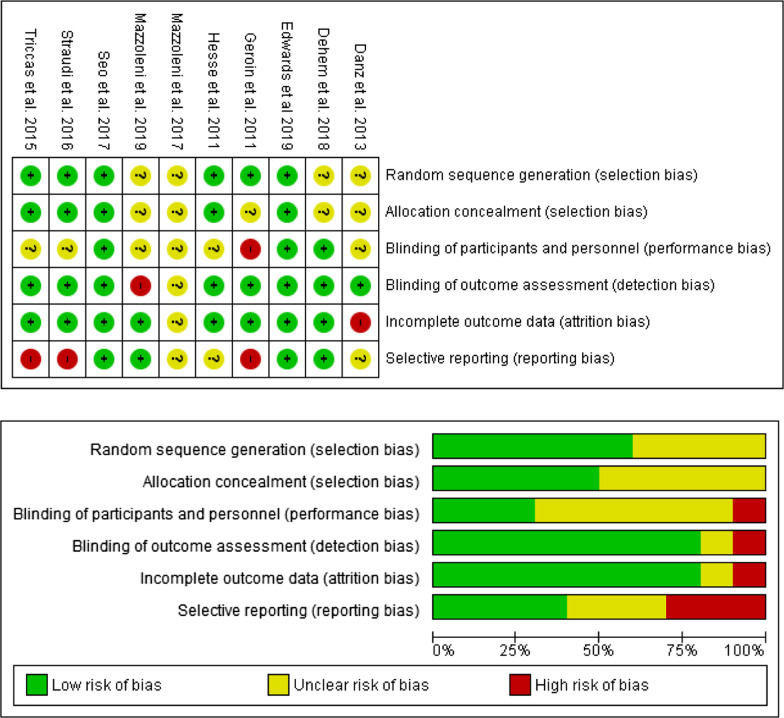
Methods: A search for randomized controlled trials (RCTs) published prior to July 15, 2021 was performed. The main outcome was function assessed with the Fugl-Meyer motor assessment for upper extremities (FM/ue) and 10-m walking test (10MWT) for the lower limbs. As secondary outcomes, strength was assessed with the Motricity Index (MI) or Medical Research Council scale (MRC), spasticity with the modified Ashworth scale (MAS), functional independence with the Barthel Index (BI), and kinematic parameters.
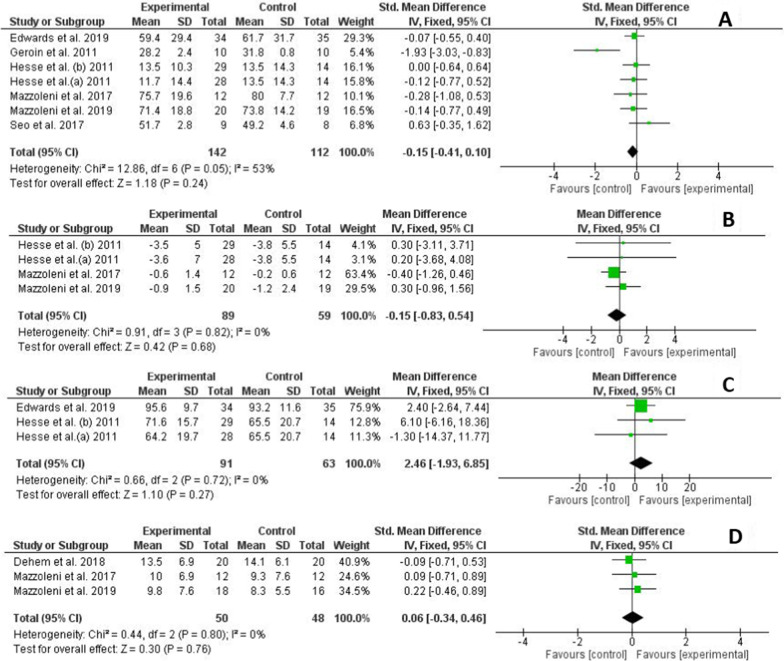
Results: Ten studies were included for analysis (n = 368 enrolled participants). The results showed a non-significant effect for tDCS combined with RT to improve upper limb function [standardized mean difference (SMD) = - 0.12; 95% confidence interval (CI): - 0.35-0.11)]. However, a positive effect of the combined therapy was observed in the lower limb function (SMD = 0.48; 95% CI: - 0.15-1.12). Significant results favouring tDCS combined with RT were not found in strength (SMD = - 0.15; 95% CI: - 0.4-0.1), spasticity [mean difference (MD) = - 0.15; 95% CI: - 0.8-0.5)], functional independence (MD = 2.5; 95% CI: - 1.9-6.9) or velocity of movement (SMD = 0.06; 95% CI: - 0.3-0.5) with a "moderate" or "low" recommendation level according to the GRADE guidelines.
Conclusions: Current findings suggest that tDCS combined with RT does not improve upper limb function, strength, spasticity, functional independence or velocity of movement after stroke. However, tDCS may enhance the effects of RT alone for lower limb function. tDCS parameters and the stage or type of stroke injury could be crucial factors that determine the effectiveness of this therapy.
Keywords: Neuromodulation; Robotic; Stroke; Transcranial direct current stimulation; tDCS.
© 2021. The Author(s).
Conflict of interest statement
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures



References
-
- Feigin VL, Abajobir AA, Abate KH, Abd-Allah F, Abdulle AM, Abera SF, et al. Global, regional, and national burden of neurological disorders during 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Neurol. 2017;16(11):877–897. doi: 10.1016/S1474-4422(17)30299-5. - DOI - PMC - PubMed
-
- Prynn JE, Kuper H. Perspectives on disability and non-communicable diseases in low-and middle-income countries, with a focus on stroke and dementia. Int J Environ Res Public Health. 2019;16: 3488. https://www.mdpi.com/1660-4601/16/18/3488. Accessed 8 May 2020. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
