

Lung transplantation: how we do it
- PMID: 34566281
- PMCID: PMC8448665
- DOI: 10.1007/s12055-021-01218-w
Lung transplantation: how we do it
Abstract
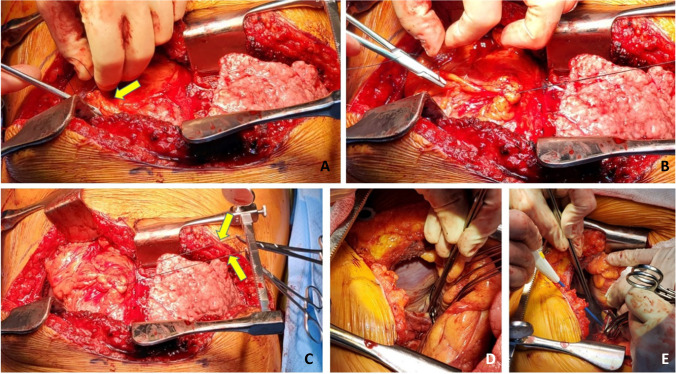
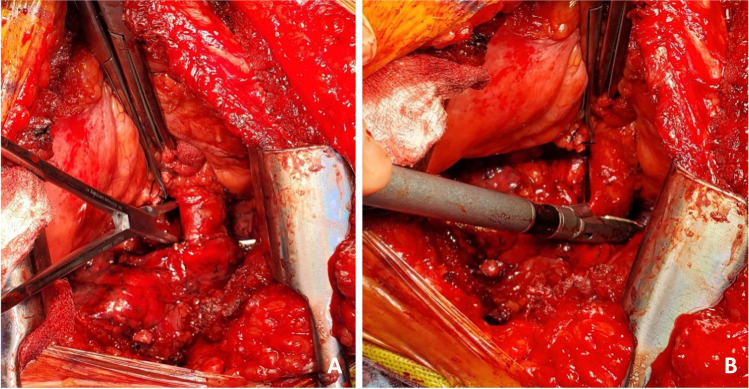
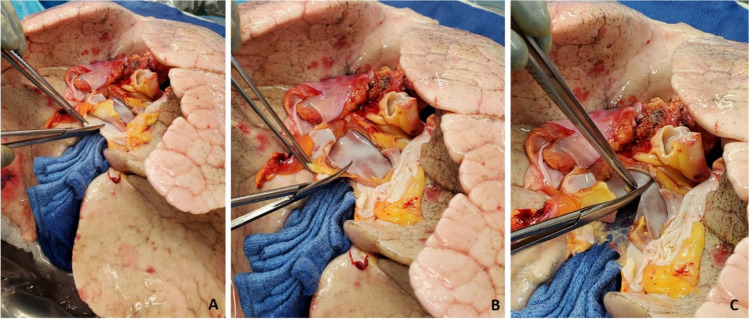
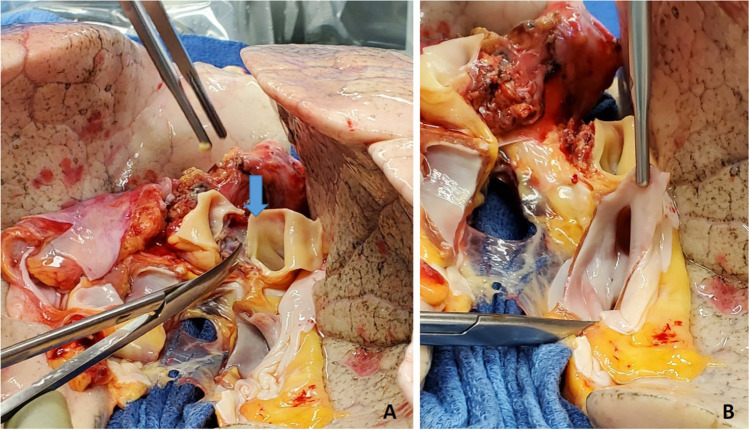
Lung transplantation is considered the gold standard for patients with chronic end-stage pulmonary disease. However, due to the complexity of management and relatively lower median survival as compared to other solid organs, many programs across the world have been slow to adopt the same. In our institution, we started lung transplantation in September 1990. And since then, we performed close to 900 lung transplantations. Here, we describe in detail the operative steps adopted in our institution for a successful lung transplantation. There have been very few variations over the years. We believe that having a standardized technique is one of the important features for success of a lung transplant program.
Keywords: End-stage pulmonary disease; Lung transplantation; Operative technique.
© The Author(s) 2021.
Conflict of interest statement
Conflict of interestThe authors declare no competing interests.
Figures


























References
-
- Lonchyna VA. Single lung transplantation. Operative Tech Thorac Cardiovasc Surg. 1999;4:142–161. doi: 10.1016/S1522-2942(07)70111-3. - DOI
Publication types
LinkOut - more resources
Full Text Sources