

FHR-5 Serum Levels and CFHR5 Genetic Variations in Patients With Immune Complex-Mediated Membranoproliferative Glomerulonephritis and C3-Glomerulopathy
- PMID: 34566977
- PMCID: PMC8461307
- DOI: 10.3389/fimmu.2021.720183
FHR-5 Serum Levels and CFHR5 Genetic Variations in Patients With Immune Complex-Mediated Membranoproliferative Glomerulonephritis and C3-Glomerulopathy
Abstract
Background: Factor H-related protein 5 (FHR-5) is a member of the complement Factor H protein family. Due to the homology to Factor H, the main complement regulator of the alternative pathway, it may also be implicated in the pathomechanism of kidney diseases where Factor H and alternative pathway dysregulation play a role. Here, we report the first observational study on CFHR5 variations along with serum FHR-5 levels in immune complex-mediated membranoproliferative glomerulonephritis (IC-MPGN) and C3 glomerulopathy (C3G) patients together with the clinical, genetic, complement, and follow-up data.
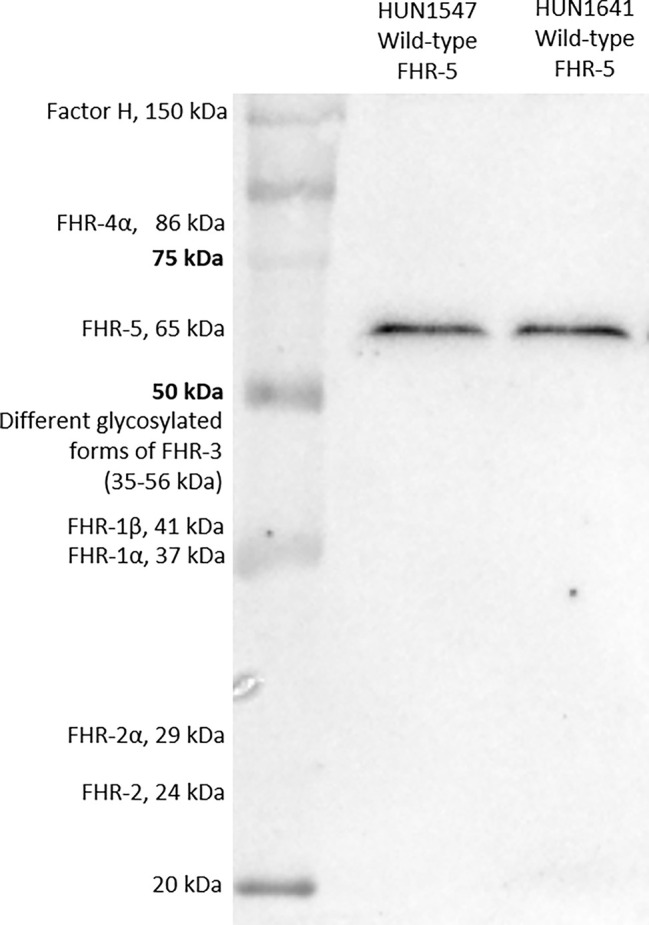
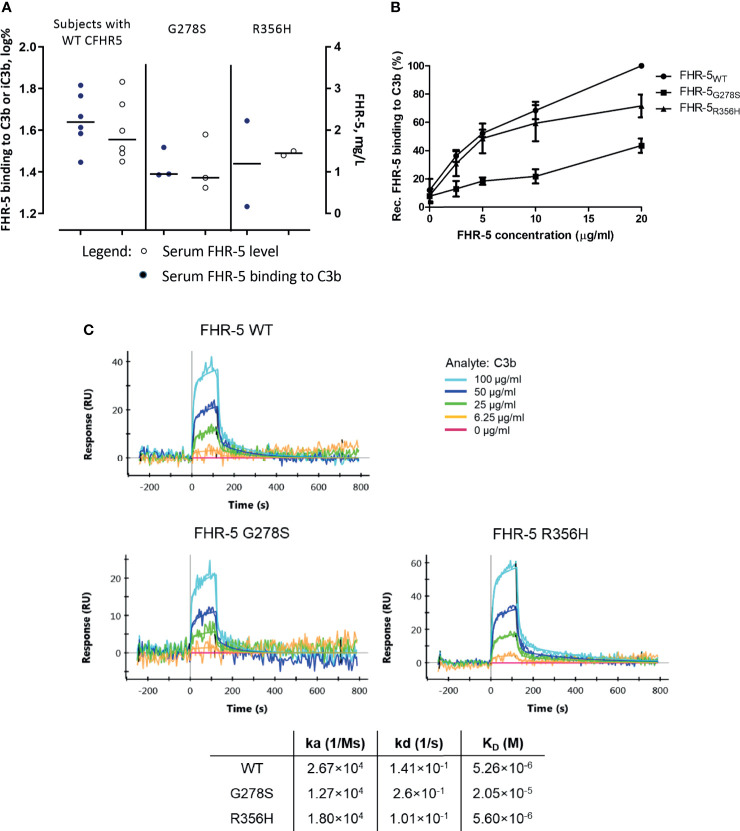
Methods: A total of 120 patients with a histologically proven diagnosis of IC-MPGN/C3G were enrolled in the study. FHR-5 serum levels were measured in ELISA, the CFHR5 gene was analyzed by Sanger sequencing, and selected variants were studied as recombinant proteins in ELISA and surface plasmon resonance (SPR).
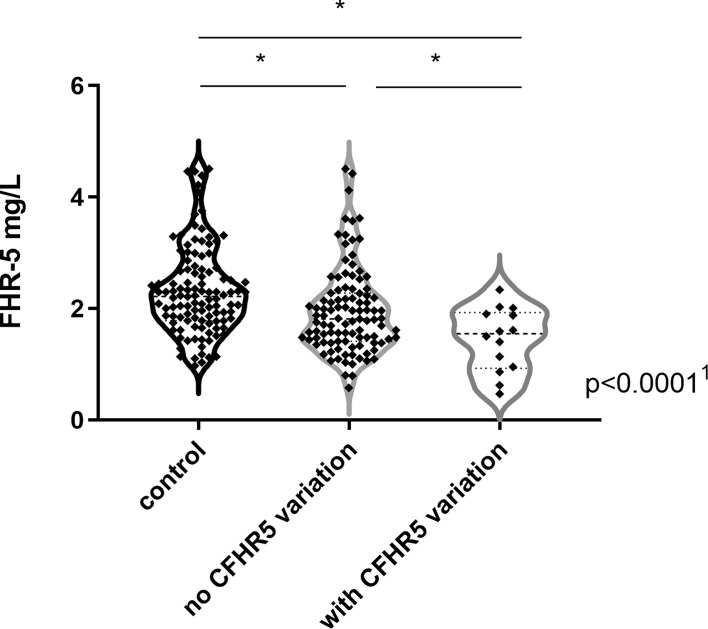
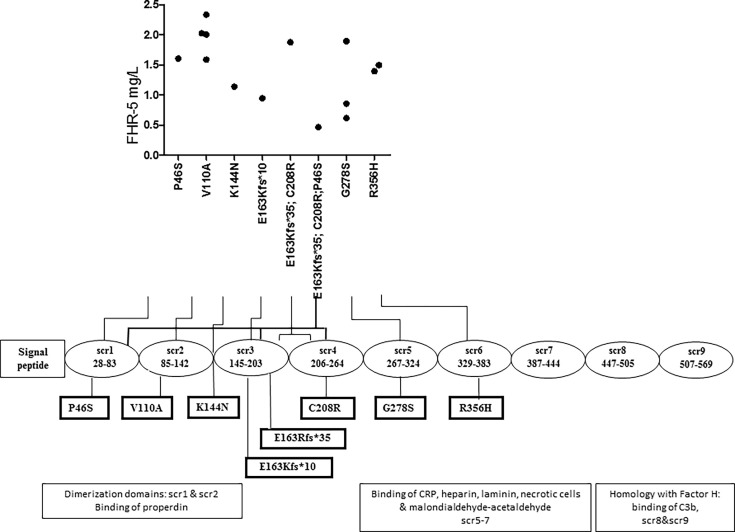
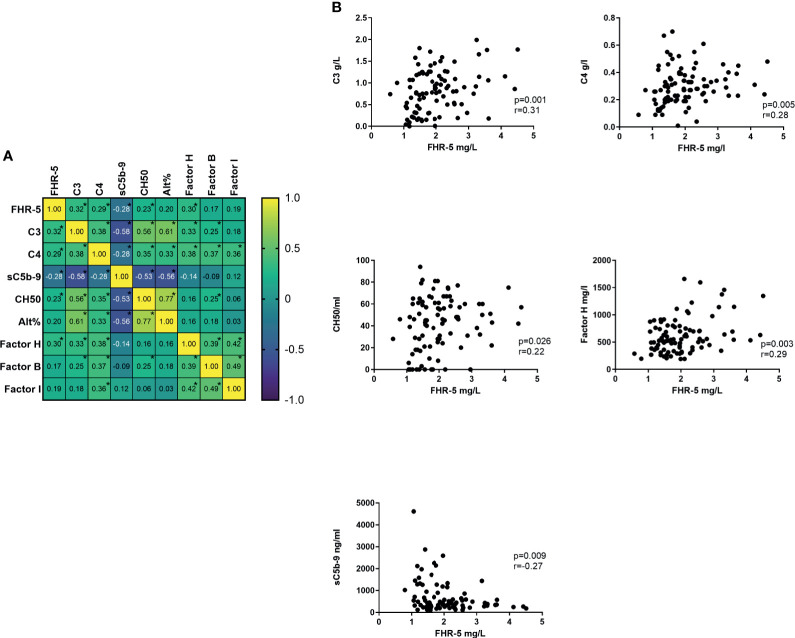
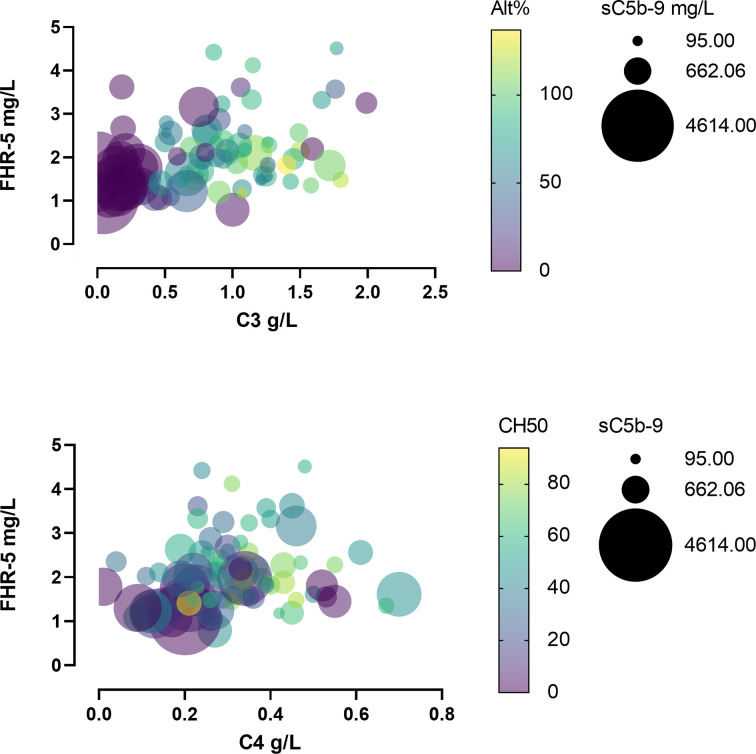
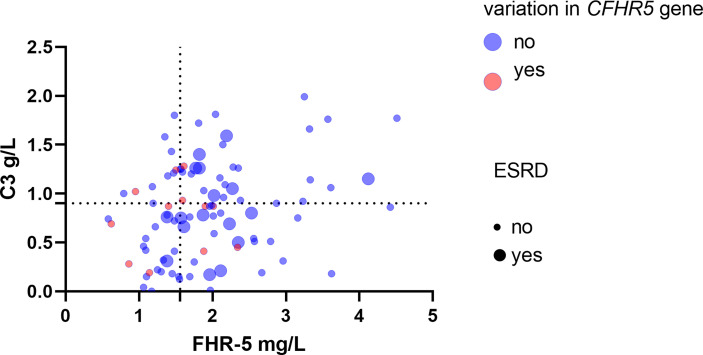
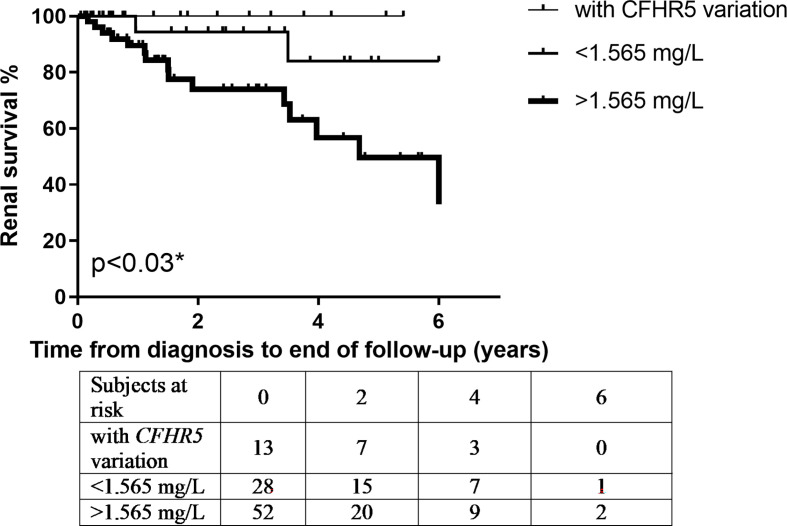
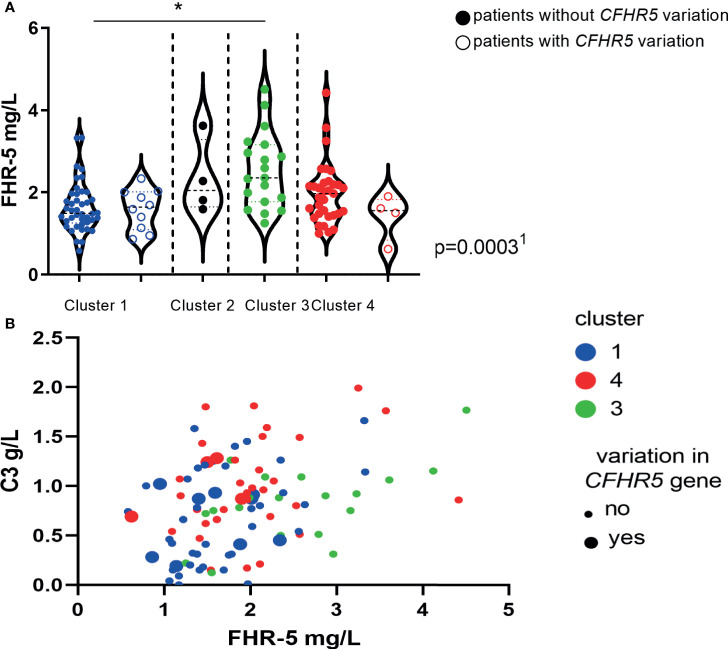
Results: Eight exonic CFHR5 variations in 14 patients (12.6%) were observed. Serum FHR-5 levels were lower in patients compared to controls. Low serum FHR-5 concentration at presentation associated with better renal survival during the follow-up period; furthermore, it showed clear association with signs of complement overactivation and clinically meaningful clusters.
Conclusions: Our observations raise the possibility that the FHR-5 protein plays a fine-tuning role in the pathogenesis of IC-MPGN/C3G.
Keywords: C3 glomerulonephritis (C3GN); C3 glomerulopathy; dense deposit disease (DDD); immune complex-mediated glomerulonephritis; membranoproliferative glomerulonephritis.
Copyright © 2021 Garam, Cserhalmi, Prohászka, Szilágyi, Veszeli, Szabó, Uzonyi, Iliás, Aigner, Schmidt, Gaggl, Sunder-Plassmann, Bajcsi, Brunner, Dumfarth, Cejka, Flaschberger, Flögelova, Haris, Hartmann, Heilos, Mueller, Rusai, Arbeiter, Hofer, Jakab, Sinkó, Szigeti, Bereczki, Janko, Kelen, Reusz, Szabó, Klenk, Kóbor, Kojc, Knechtelsdorfer, Laganovic, Lungu, Meglic, Rus, Kersnik Levart, Macioniene, Miglinas, Pawłowska, Stompór, Podracka, Rudnicki, Mayer, Rysava, Reiterova, Saraga, Seeman, Zieg, Sládková, Stajic, Szabó, Capitanescu, Stancu, Tisljar, Galesic, Tislér, Vainumäe, Windpessl, Zaoral, Zlatanova, Józsi and Csuka.
Conflict of interest statement
Author VJ was employed by company Medimpax. The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous