

Imaging update on soft tissue sarcoma
- PMID: 34567971
- PMCID: PMC8449057
- DOI: 10.1016/j.jcot.2021.101568
Imaging update on soft tissue sarcoma
Abstract
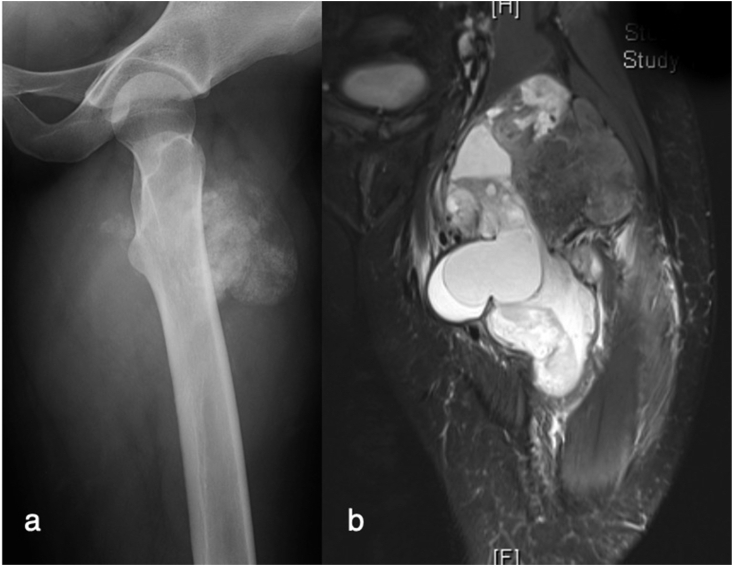
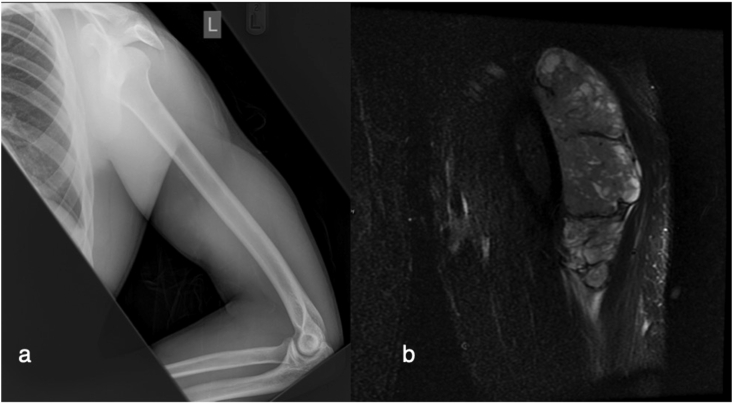
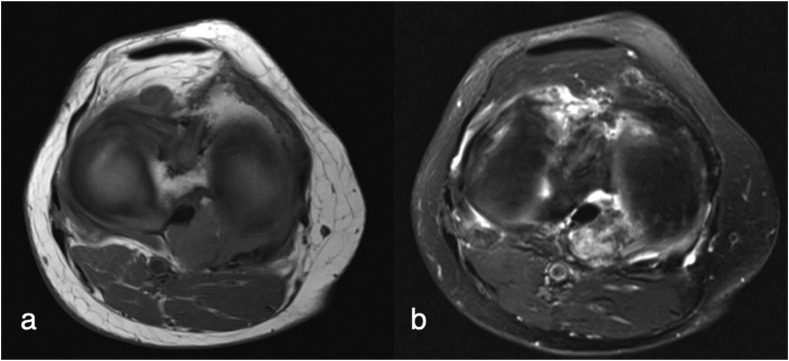
Soft tissue sarcomas (STS) are rare tumours presenting as soft tissue lumps. Ultrasound is often the primary modality for the initial assessment, with MRI the mainstay for lesion characterisation. PET/CT along with other emerging MRI sequences are used in certain situations as an adjunct and problem solving tool in STS staging and assessment of disease recurrence. Recent advances include the promise of whole body MRI, hybrid PET/MRI, diffusion weighted imaging, dynamic contrast enhanced MRI and advances in artificial intelligence. This article discusses current concepts in extremity STS imaging and highlights recent advances.
Keywords: Advances or current concepts or imaging concepts; CT, computed tomography; DCE-MRI, dynamic contrast enhanced magnetic resonance imaging; DWI, diffusion weighted imaging; FDG, fluorodeoxyglucose; Imaging or radiology or musculoskeletal radiology or MSK Radiology; MRI, magnetic resonance imaging; MSK, musculoskeletal; PET, positron emission tomography; STS, soft tissue sarcoma; Soft tissue sarcoma or soft tissue sarcomas or STS or STSs or sarcoma or sarcomas; Ultrasound or magnetic resonance imaging or MRI or PET-CT or CT or Computed tomography or X-Ray or contrast enhanced ultrasound or CEUS or Diffusion weighted imaging or DWI or Dynamic contrast enhancement or DCE-MRI or whole body MRI; WBMRI, whole body MRI.
© 2021 Delhi Orthopedic Association. All rights reserved.
Figures















References
-
- Cancer.org Key statistics for soft tissue sarcomas. 2021. https://www.cancer.org/cancer/soft-tissue-sarcoma/about/key-statistics.html [online] Available at:
-
- Improving Outcomes for People with Sarcoma | Guidance. NICE; 2006. https://www.nice.org.uk/guidance/csg9 Nice.org.uk. Published.
-
- Belli P., Costantini M., Mirk P., Maresca G., Priolo F., Marano P. Role of color Doppler sonography in the assessment of musculoskeletal soft tissue masses [published correction appears in J Ultrasound Med 2001 May;20(5):516] J Ultrasound Med. 2000;19(12):823–830. doi: 10.7863/jum.2000.19.12.823. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources