

Off-Label Underdosing or Overdosing of Non-vitamin K Antagonist Oral Anticoagulants in Patients With Atrial Fibrillation: A Meta-Analysis
- PMID: 34568462
- PMCID: PMC8455833
- DOI: 10.3389/fcvm.2021.724301
Off-Label Underdosing or Overdosing of Non-vitamin K Antagonist Oral Anticoagulants in Patients With Atrial Fibrillation: A Meta-Analysis
Abstract
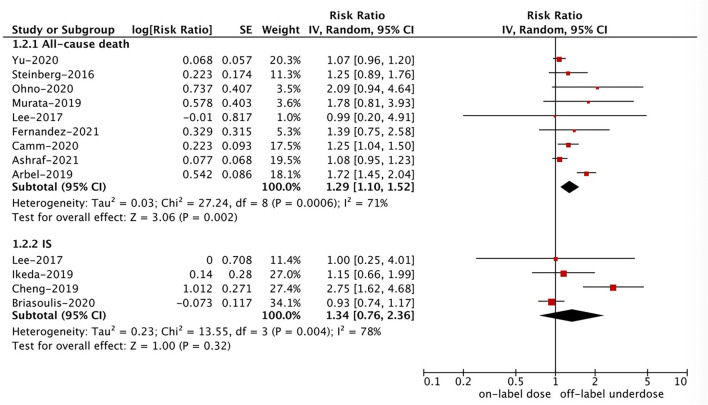
Background: Several studies have investigated the role of off-label non-vitamin K antagonist oral anticoagulants (NOACs) in patients with atrial fibrillation (AF). We aimed to compare the effectiveness and safety outcomes between off-label underdose or overdose vs. on-label dose of NOACs in AF patients. Methods: The PubMed database was systematically searched until August 2021. Observational cohorts were included if they compared the outcomes of off-label underdose or overdose with on-label dose of NOACs in AF patients. The risk ratios (RRs) and 95% confidence intervals (CIs) were pooled using a fixed-effects model (I 2 ≤ 50%) or a random-effects model (I 2 > 50%). Results: A total of 15 observational studies were included. Compared with on-label dose of NOACs, off-label underdose of NOACs was associated with increased risks of stroke or systemic embolism (RR = 1.09, 95% CI 1.02-1.16), and all-cause death (RR = 1.29, 95% CI 1.10-1.52) but not ischemic stroke (RR = 1.34, 95% CI 0.76-2.36), myocardial infarction (RR = 1.08, 95% CI 0.92-1.28), major bleeding (RR = 0.97, 95% CI 0.89-1.05), intracranial hemorrhage (RR = 1.12, 95% CI 0.90-1.40), and gastrointestinal bleeding (RR = 0.96, 95% CI 0.85-1.07), whereas off-label overdose of NOACs was associated with increased risks of SSE (RR = 1.20, 95% CI 1.05-1.36), all-cause death (RR = 1.22, 95% CI 1.06-1.39), and major bleeding (RR = 1.33, 95% CI 1.16-1.52) but not gastrointestinal bleeding (RR = 1.18, 95% CI 0.99-1.42) and myocardial infarction (RR = 0.98, 95% CI 0.75-1.30). Conclusion: Compared with on-label dose of NOACs, off-label underdose was associated with increased risks of stroke or systemic embolism and all-cause death, whereas off-label overdose of NOACs was associated with increased risks of stroke or systemic embolism, all-cause death, and major bleeding.
Keywords: anticoagulants; atrial fibrillation; meta-analysis; off label; outcomes.
Copyright © 2021 Wu, Hu, Liu and Gu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
Off-label dosing of non-vitamin K antagonist oral anticoagulants and clinical outcomes in Asian patients with atrial fibrillation.Heart Rhythm. 2020 Dec;17(12):2102-2110. doi: 10.1016/j.hrthm.2020.07.022. Epub 2020 Jul 20. Heart Rhythm. 2020. PMID: 32702416
-
Effect of non-vitamin K antagonist oral anticoagulants versus warfarin in heart failure patients with atrial fibrillation.Heart Fail Rev. 2021 Nov;26(6):1391-1397. doi: 10.1007/s10741-020-09946-8. Heart Fail Rev. 2021. PMID: 32249407 Review.
-
Non-Vitamin K Antagonist Oral Anticoagulants Versus Warfarin in Patients with Atrial Fibrillation with Coronary or Peripheral Artery Disease.Int Heart J. 2020 Mar 28;61(2):231-238. doi: 10.1536/ihj.19-202. Epub 2020 Mar 14. Int Heart J. 2020. PMID: 32173695
-
Non-Vitamin K Antagonist Oral Anticoagulants Versus Warfarin in Asians With Atrial Fibrillation: Meta-Analysis of Randomized Trials and Real-World Studies.Stroke. 2019 Oct;50(10):2819-2828. doi: 10.1161/STROKEAHA.119.026054. Epub 2019 Aug 19. Stroke. 2019. PMID: 31422735 Free PMC article.
-
Real-world comparisons of reduced-dose non-vitamin K antagonist oral anticoagulants versus warfarin in atrial fibrillation: a systematic review and meta-analysis.Heart Fail Rev. 2020 Nov;25(6):973-983. doi: 10.1007/s10741-019-09887-x. Heart Fail Rev. 2020. PMID: 31713086
Cited by
-
Important Risk Factors in Patients with Nonvalvular Atrial Fibrillation Taking Dabigatran Using Integrated Machine Learning Scheme-A Post Hoc Analysis.J Pers Med. 2022 May 6;12(5):756. doi: 10.3390/jpm12050756. J Pers Med. 2022. PMID: 35629177 Free PMC article.
-
Current Real-World Status of Off-Label Under- and Over-Dose of Direct Oral Anticoagulants After Atrial Fibrillation Ablation.J Cardiovasc Electrophysiol. 2025 Mar;36(3):564-575. doi: 10.1111/jce.16560. Epub 2025 Jan 7. J Cardiovasc Electrophysiol. 2025. PMID: 39777770 Free PMC article.
-
Direct-Acting Oral Anticoagulants and Potential Inconsistencies with FDA-Approved Dosing for Non-Valvular Atrial Fibrillation: A Retrospective Real-World Analysis Across Nine US Healthcare Systems.J Gen Intern Med. 2025 Mar;40(4):828-837. doi: 10.1007/s11606-024-09106-w. Epub 2024 Oct 18. J Gen Intern Med. 2025. PMID: 39424771 Free PMC article.
-
Comparative Effectiveness and Safety of Off-Label Underdosed Direct Oral Anticoagulants in Asian Patients with Atrial Fibrillation: A Systematic Review and Meta-analysis.Drug Saf. 2025 Jan;48(1):25-42. doi: 10.1007/s40264-024-01476-8. Epub 2024 Aug 30. Drug Saf. 2025. PMID: 39214955
-
Apixaban outcomes in atrial fibrillation patients with a single-dose reduction criterion: ASPIRE 1-year results.Eur Heart J Cardiovasc Pharmacother. 2025 Aug 12;11(5):403-411. doi: 10.1093/ehjcvp/pvaf018. Eur Heart J Cardiovasc Pharmacother. 2025. PMID: 40113236 Free PMC article.
References
-
- January CT, Wann LS, Calkins H, Chen LY, Cigarroa JE, Cleveland JC, et al. . 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines and the heart rhythm society in collaboration with the society of thoracic surgeons. Circulation. (2019). 140:R665. 10.1161/CIR.0000000000000665 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources