

Review of evidences for management of rapid sequence spinal anesthesia for category one cesarean section, in resource limiting setting
- PMID: 34568612
- PMCID: PMC7470710
- DOI: 10.1016/j.ijso.2020.08.013
Review of evidences for management of rapid sequence spinal anesthesia for category one cesarean section, in resource limiting setting
Abstract
Background: Globally obstetric anesthesia is being done under spinal and epidural than general anesthesia (GA) for most caesarean sections (CSs). This is because GA is associated with failed endotracheal intubation and aspiration of gastric contents. Eventhough general anesthesia is the fastest method for anesthetizing a category 1 cesarean section, it is associated with increased maternal mortality and morbidity. Spinal anesthesia is the preferred regional technique for cesarean section but failure sometimes occurs. To minimize the time factor of spinal anesthesia as well as to avoid the side effects of general anesthesia 'rapid sequence spinal '(RSS) has developed as a novel approach in cases of category one cesarean sections.
Methods: The study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol. Search engines like PubMed through HINARI, Cochrane database and Google Scholars were used to find high-level evidences that help to draw appropriate conclusions.
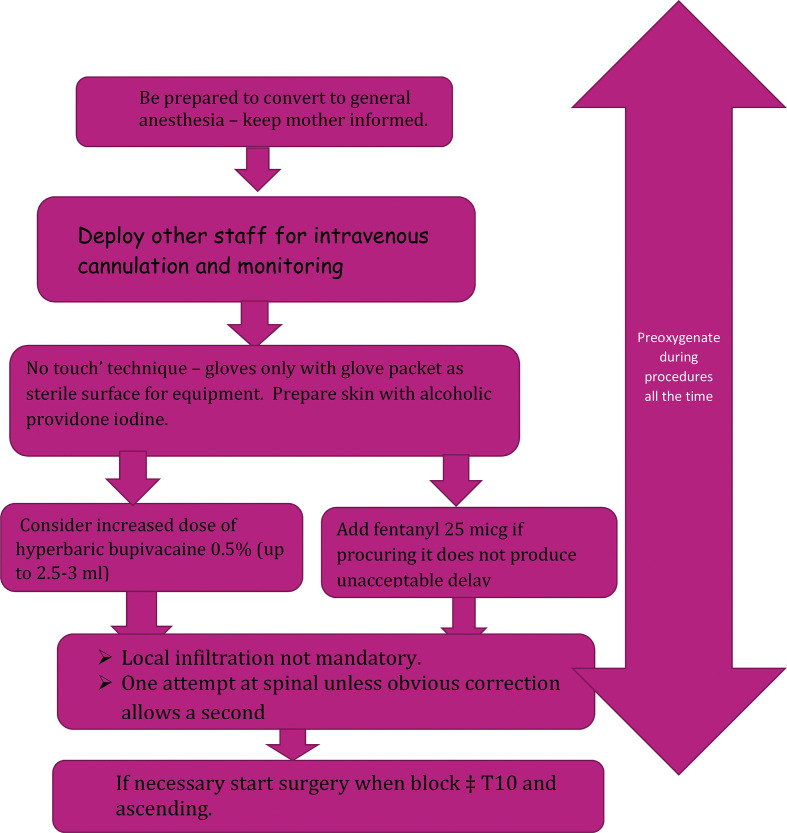
Discussion: Neuraxial anesthetic techniques have several advantages which include low risk of aspiration and failed intubation, avoidance of central nervous system (CNS) and respiratory depressant drugs, the ability to maintain a wakeful state of mother enjoying the experience of delivery of baby and also lower incidence of blood loss. 'Rapid sequence spinal' described to minimize anesthetic time. This consists of a no-touch spinal technique, consideration of omission of the spinal opioid, limiting spinal attempts, allowing the start of surgery before full establishment of the spinal block, and being prepared for conversion to general anesthesia if there are delays or problems. To do rapid sequence spinal anesthesia safely and timely, cooperative work is mandatory with good team relation for those simultaneous and necessary tasks.
Conclusion: The choice of anesthetic in Cesarean section has long been recognized as one of prime importance, because there are two lives to safeguard instead of one. A balance must be struck between the anesthetic dictated by the general condition of the mother and that suited to the needs of the fetal respiratory system.
Keywords: Cesarean section; Difficult intubation; Fetal distress; Rapid sequence spinal anesthesia.
© 2020 The Author(s).
Figures
References
-
- Kinsella S., Girgirah K., Scrutton M. Rapid sequence spinal anaesthesia for category-1 urgency caesarean section: a case series. Anaesthesia. 2010;65(7):664–669. - PubMed
-
- Bhattacharya S., Ghosh S., Chattopadhya U., Saha D., Bisai S., Saha M. Rapid sequence spinal anesthesia versus general anesthesia: a prospective randomized study of anesthesia to delivery time in category-1 caesarean section. Journal of Obstetric Anaesthesia and Critical Care. 2016;6(2):75.
-
- Chiron B., Laffon M., Ferrandiere M., Pittet J.-F., Marret H., Mercier C. Standard preoxygenation technique versus two rapid techniques in pregnant patients. Int J Obstet Anesth. 2004;13(1):11–14. - PubMed
-
- Mhyre J.M., Riesner M.N., Polley L.S., Naughton N.N. A series of anesthesia-related maternal deaths in Michigan, 1985–2003. Anesthesiology: The Journal of the American Society of Anesthesiologists. 2007;106(6):1096–1104. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical