

Termination Based on Event Accrual in Per Protocol Versus Intention to Treat in the ROCKET AF Trial
- PMID: 34569249
- PMCID: PMC8649140
- DOI: 10.1161/JAHA.121.022485
Termination Based on Event Accrual in Per Protocol Versus Intention to Treat in the ROCKET AF Trial
Abstract
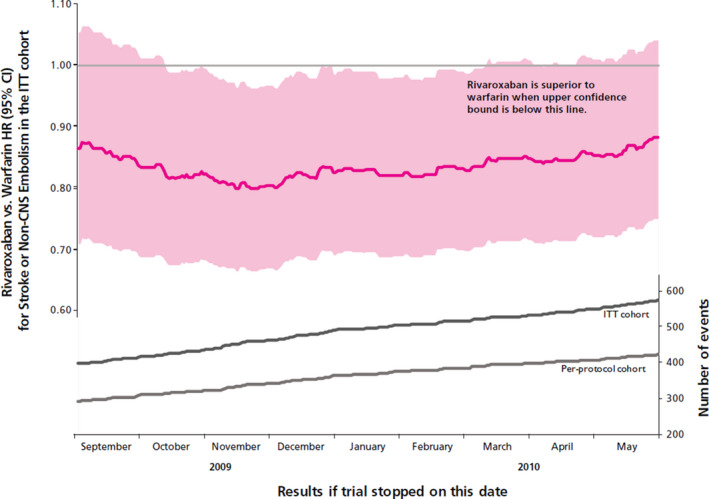
Background In event-driven clinical trials, study termination is based on accrual of a target number of primary efficacy events. For noninferiority trials in which superiority is conditionally examined, the ideal cohort in which to track event accrual is unclear. We used data from the ROCKET AF (Rivaroxaban Once Daily Oral Direct Factor Xa Inhibition Compared With Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation) trial to determine the effect of primary efficacy-event tracking in the per-protocol cohort during the on-treatment period versus the intention-to-treat (ITT) cohort during the ITT period. Methods and Results ROCKET AF was terminated after accruing 429 primary efficacy events (stroke or systemic embolism) in the per-protocol cohort during the on-treatment period for noninferiority. We identified the date on which 429 events occurred in the ITT cohort during the ITT period. We performed noninferiority and superiority analyses based on hypothetical study termination on this date. ROCKET AF would have terminated 226 days earlier if events were tracked during the ITT period. Similar to the main trial findings, rivaroxaban would have met noninferiority versus warfarin for the primary efficacy end point (hazard ratio [HR], 0.77; 95% CI, 0.62-0.96; P<0.001). In contrast to the main trial findings, rivaroxaban would have met superiority for the primary efficacy end point (HR, 0.82; 95% CI, 0.68-0.99; P=0.038). In both termination scenarios, rivaroxaban was associated with a lower risk of intracranial hemorrhage and similar risk of other safety end points. Conclusions Clinical trial termination based on event accrual in the ITT cohort versus the per-protocol cohort may have important implications on trial results depending on rates of study drug discontinuation and event rates off treatment.
Keywords: anticoagulation; atrial fibrillation; clinical trial; embolic stroke; research methodology; warfarin.
Conflict of interest statement
Dr Becker reports research funding from the National Institutes of Health and scientific advisory and data safety and monitoring board consulting fees from Ionis, Akcea, Basking, and Novartis. Dr Berkowitz was employed as a clinical research physician at Bayer during the design and operationalization of the ROCKET AF trial. Dr Breithardt reports consulting fees from Bayer HealthCare, Johnson & Johnson, Boehringer Ingelheim, Sanofi‐Aventis, MSD, and 3M. Dr Califf reports employment from Verily and Google Health, and consulting/advisory board fees from Cytokinetics, United Medicines, and Clinetic. Dr Carnicelli reports research funding from the National Institutes of Health. Dr Fox reports grant funding and consulting fees from Bayer/Janssen (related to ROCKET AF), grant funding from AstraZeneca (unrelated), and consulting fees from Sanofi/Regeneron and Verseon (unrelated). Dr Halperin reports consulting fees from the sponsor of ROCKET AF trial and modest consulting fees from the Colorado Prevention Center as a member of the ATLAS group. Dr Hankey reports personal fees from Duke University during the conduct of the study, and personal fees from the American Heart Association and personal fees from Bayer outside the submitted work. Dr Mahaffey reports research grants/contracts from Afferent, American Heart Association, Amgen, Apple, AstraZeneca, Bayer, Cardiva Medical, Eidos, Ferring, Gilead, Google (Verily), Johnson & Johnson, Luitpold, Medtronic, Merck, National Institutes of Health, Novartis, Sanifit, Sanofi, and St. Jude, and consulting fees from Abbott, Amgen, Anthos, AstraZeneca, Baim Institute, Bayer, Boehringer Ingelheim, CSL Behring, Elsevier, Inova, Intermountain Health, Johnson & Johnson, Medscape, Mount Sinai, Mundi Pharma, Myokardia, National Institutes of Health, Novartis, Novo Nordisk, Otsuka, Portola, Regeneron, Sanofi, SmartMedics, and Theravance. Dr Nessel reports employment from Janssen Research & Development. Dr Patel reports research funding from Bayer, Janssen, Heartflow, and the National Heart, Lung, and Blood Institute, and consulting fees from Bayer and Janssen. Dr Piccini reports grants for clinical research from Abbott, American Heart Association, Association for the Advancement of Medical Instrumentation, Bayer, Boston Scientific, and Philips, and serves as a consultant to Abbott, Allergan, ARCA Biopharma, Biotronik, Boston Scientific, LivaNova, Medtronic, Milestone, Myokardia, Sanofi, and Philips. Dr Singer reports grant funding from Bristol Myers Squibb (significant) and consulting fees from Boehringer Ingelheim (modest), Bristol Myers Squibb (significant), Fitbit (significant), Johnson and Johnson (modest), Merck (modest), and Pfizer (modest). A.S. Hellkamp has no disclosures to report.
Figures



References
-
- ROCKET AF Study Investigators . Rivaroxaban‐once daily, oral, direct factor Xa inhibition compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation: rationale and design of the ROCKET AF study. Am Heart J. 2010;159:340–347 e1. doi: 10.1016/j.ahj.2009.11.025 - DOI - PubMed
-
- US Department of Health and Human Services, Food and Drug Administration . Non‐Inferiority Clinical Trials to Establish Effectiveness: Guidance for Industry. 2016. Available at: https://www.fda.gov/regulatory‐information/search‐fda‐guidance‐documents.... Accessed September 6, 2021.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
