

Impact of Navigation on 30-Day Outcomes for Adult Spinal Deformity Surgery
- PMID: 34569338
- PMCID: PMC10556894
- DOI: 10.1177/21925682211047551
Impact of Navigation on 30-Day Outcomes for Adult Spinal Deformity Surgery
Abstract
Study design: Retrospective database study.
Objective: Navigation has been increasingly used to treat degenerative disease, with positive radiographic and clinical outcomes and fewer adverse events and reoperations, despite increased operative time. However, short-term analysis on treating adult spinal deformity (ASD) surgery with navigation is limited, particularly using large nationally represented cohorts. This is the first large-scale database study to compare 30-day readmission, reoperation, morbidity, and value-per-operative time for navigated and conventional ASD surgery.
Methods: Adults were identified in the National Surgical Quality Improvement Program (NSQIP) database. Multivariate regression was used to compare outcomes between navigated and conventional surgery and to control for predictors and baseline differences.
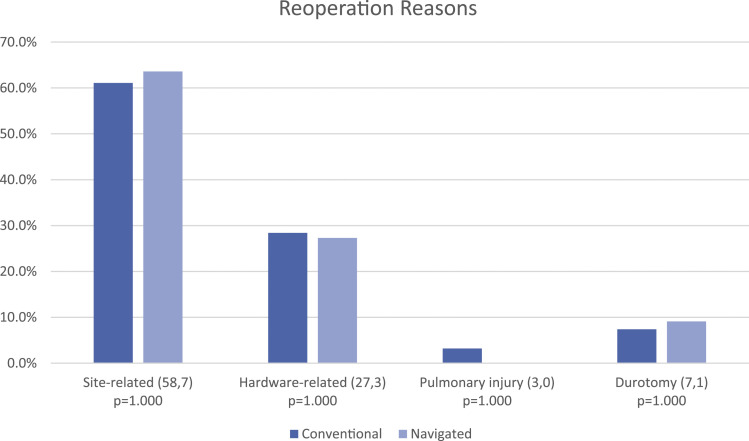
Results: 3190 ASD patients were included. Navigated and conventional patients were similar. Navigated cases had greater operative time (405 vs 320 min) and mean RVUs per case (81.3 vs 69.7), and had more supplementary pelvic fixations (26.1 vs 13.4%) and osteotomies (50.3 vs 27.7%) (P <.001).In univariate analysis, navigation had greater reoperation (9.9 vs 5.2%, P = .011), morbidity (57.8 vs 46.8%, P = .007), and transfusion (52.2 vs 41.8%, P = .010) rates. Readmission was similar (11.9 vs 8.4%). In multivariate analysis, navigation predicted reoperation (OR = 1.792, P = .048), but no longer predicted morbidity or transfusion. Most reoperations were infectious and hardware-related.
Conclusions: Despite controlling for patient-related and procedural factors, navigation independently predicted a 79% increased odds of reoperation but did not predict morbidity or transfusion. Readmission was similar between groups. This is explained, in part, by greater operative time and transfusion, which are risk factors for infection. Reoperation most frequently occurred for wound- and hardware-related reasons, suggesting navigation carries an increased risk of infectious-related events beyond increased operative time.
Keywords: complications; computer assisted navigation; deformity; fusion; infection; morbidity; readmission; reoperation; spinal navigation.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Silber receives teaching fees for Stryker. Dr. Essig receives consulting fees for Stryker and DePuy. For all remaining authors, none we declared
Figures
References
-
- Safaee MM, Ames CP, Smith JS. Epidemiology and socioeconomic trends in adult spinal deformity care. Neurosurgery. 2020;87(1):25-32. - PubMed
-
- Smith JS, Shaffrey CI, Ames CP, Lenke LG. Treatment of adult thoracolumbar spinal deformity: past, present, and future: JNSPG 75th anniversary invited review article. J Neurosurg Spine. 2019;30(5):551-567. - PubMed
-
- Schwab FJ, Blondel B, Bess S, et al.. Radiographical spinopelvic parameters and disability in the setting of adult spinal deformity: a prospective multicenter analysis. Spine. 2013;38(13):E803-E812. - PubMed
LinkOut - more resources
Full Text Sources
