

E-nside Off-the-Shelf Inner Branch Stent Graft: Technical Aspects of Planning and Implantation
- PMID: 34569343
- PMCID: PMC8928429
- DOI: 10.1177/15266028211047967
E-nside Off-the-Shelf Inner Branch Stent Graft: Technical Aspects of Planning and Implantation
Abstract
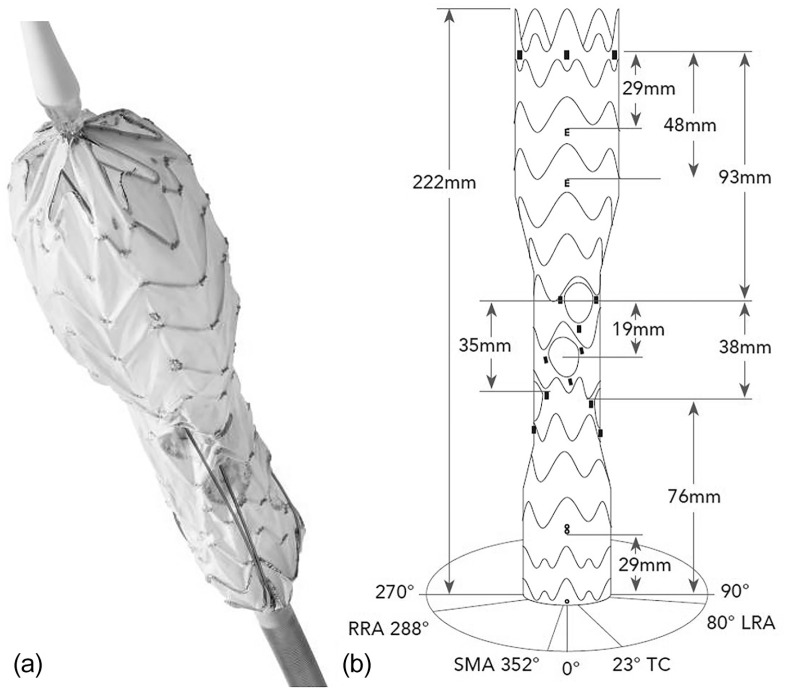
Purpose: This article aims to present all aspects regarding patient selection, planning, and implantation technique for a new off-the-shelf pre-cannulated multi-inner branch stent graft. The stent graft comes in 4 different versions with proximal diameters of 33 and 38 mm and distal diameters of 26 and 30 mm. The 4 inner branches are located in the middle segment, which has a diameter of 24 mm.
Technique: With inner branch technology, the field of application for the treatment of thoracoabdominal aortic aneurysms (TAAA) has been further extended. In addition to routine use in elective cases the pre-cannulation of the inner branches predisposes especially for emergencies. Pre-cannulation is intended to reduce the time to cannulation and the radiation dose. All steps of planning, stent-graft deployment, and cannulation of the inner branches are described in detail.
Conclusion: The E-nside stent graft represents a promising new endovascular therapy in the treatment of acute and elective TAAA. By using inner branch technology, this endograft combines the advantages of fenestrated and branched stent grafts. Indication, planning, and implantation require experience in branched and fenestrated stent graft technology.
Keywords: endograft; endovascular therapy; inner branch; off-the-shelf device; thoracoabdominal aortic aneurysm.
Conflict of interest statement
Figures




References
-
- Coselli JS, LeMaire SA, Preventza O, et al. Outcomes of 3309 thoracoabdominal aortic aneurysm repairs. J Thorac Cardiovasc Surg. 2016;151:1323–1337. - PubMed
-
- Greenberg RK, Lytle B. Endovascular repair of thoracoabdominal aneurysms. Circulation. 2008;117:2288–2296. - PubMed
-
- Tsilimparis N, Fiorucci B, Debus ES, et al. Technical aspects of implanting the t-branch off-the-shelf multibranched stent-graft for Thoracoabdominal aneurysms. J Endovasc Ther. 2017;24:397–404. - PubMed
-
- Bisdas T, Donas KP, Bosiers M, et al. Anatomical suitability of the T-branch stent-graft in patients with thoracoabdominal aortic aneurysms treated using custom-made multibranched endografts. J Endovasc Ther. 2013;20:672–677. - PubMed
-
- Bosiers MJ, Bisdas T, Donas KP, et al. Early experience with the first commercially available off-the-shelf multibranched endograft (t-branch) in the treatment of thoracoabdominal aortic aneurysms. J Endovasc Ther. 2013;20:719–725. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
