

Effect of Whole-Genome Sequencing on the Clinical Management of Acutely Ill Infants With Suspected Genetic Disease: A Randomized Clinical Trial
- PMID: 34570182
- PMCID: PMC8477301
- DOI: 10.1001/jamapediatrics.2021.3496
Effect of Whole-Genome Sequencing on the Clinical Management of Acutely Ill Infants With Suspected Genetic Disease: A Randomized Clinical Trial
Erratum in
-
Error in Introduction.JAMA Pediatr. 2021 Dec 1;175(12):1295. doi: 10.1001/jamapediatrics.2021.5326. JAMA Pediatr. 2021. PMID: 34870712 Free PMC article. No abstract available.
Abstract
Importance: Whole-genome sequencing (WGS) shows promise as a first-line genetic test for acutely ill infants, but widespread adoption and implementation requires evidence of an effect on clinical management.
Objective: To determine the effect of WGS on clinical management in a racially and ethnically diverse and geographically distributed population of acutely ill infants in the US.
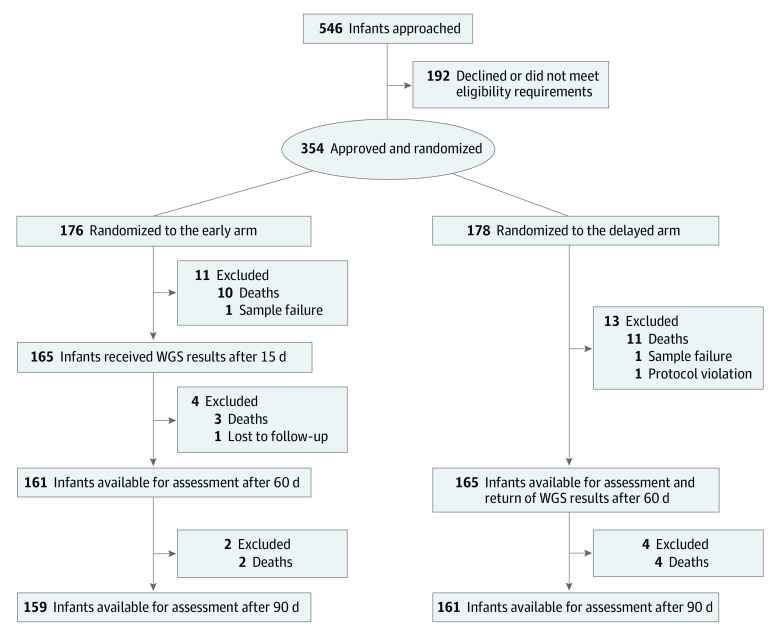
Design, setting, and participants: This randomized, time-delayed clinical trial enrolled participants from September 11, 2017, to April 30, 2019, with an observation period extending to July 2, 2019. The study was conducted at 5 US academic medical centers and affiliated children's hospitals. Participants included infants aged between 0 and 120 days who were admitted to an intensive care unit with a suspected genetic disease. Data were analyzed from January 14 to August 20, 2020.
Interventions: Patients were randomized to receive clinical WGS results 15 days (early) or 60 days (delayed) after enrollment, with the observation period extending to 90 days. Usual care was continued throughout the study.
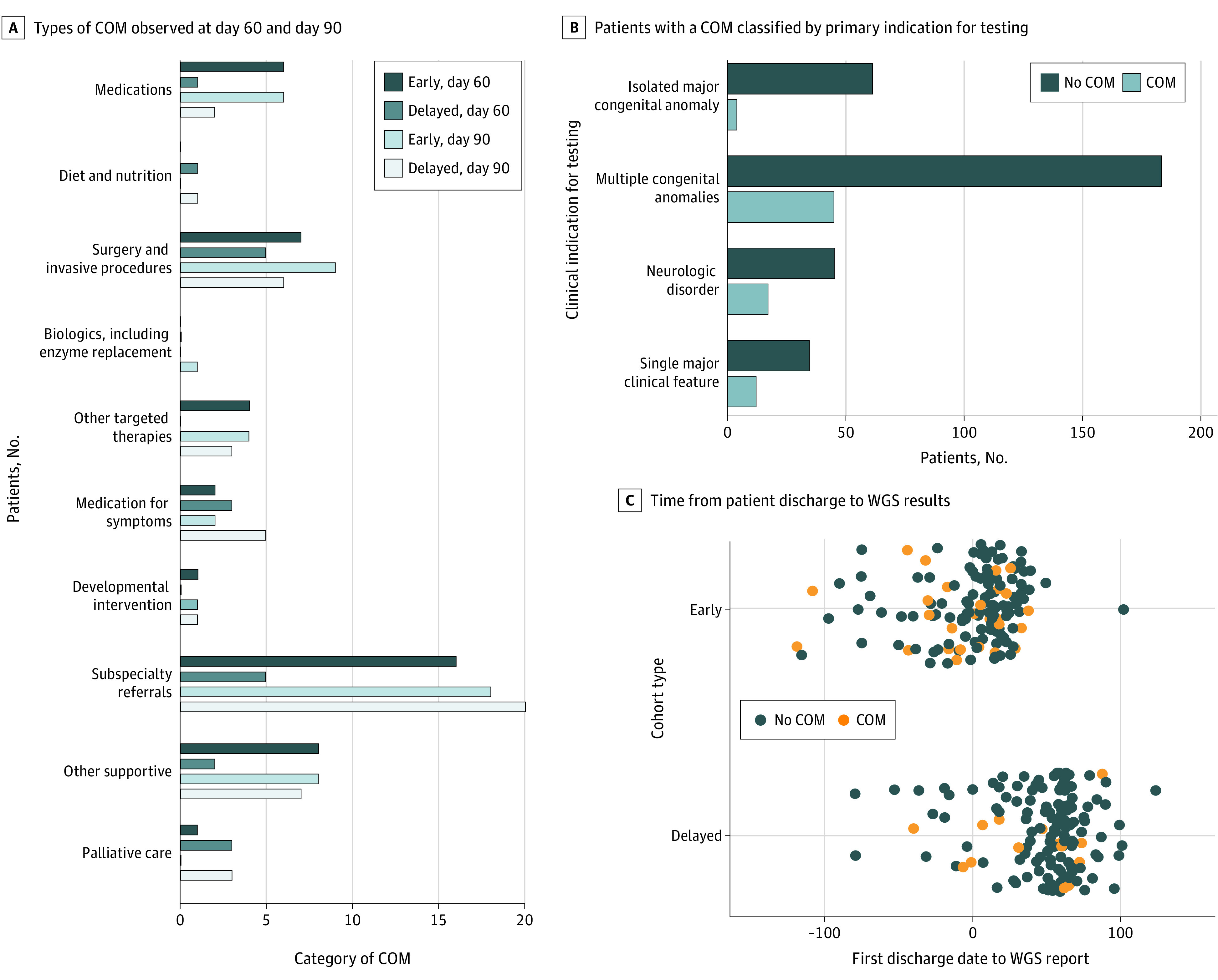
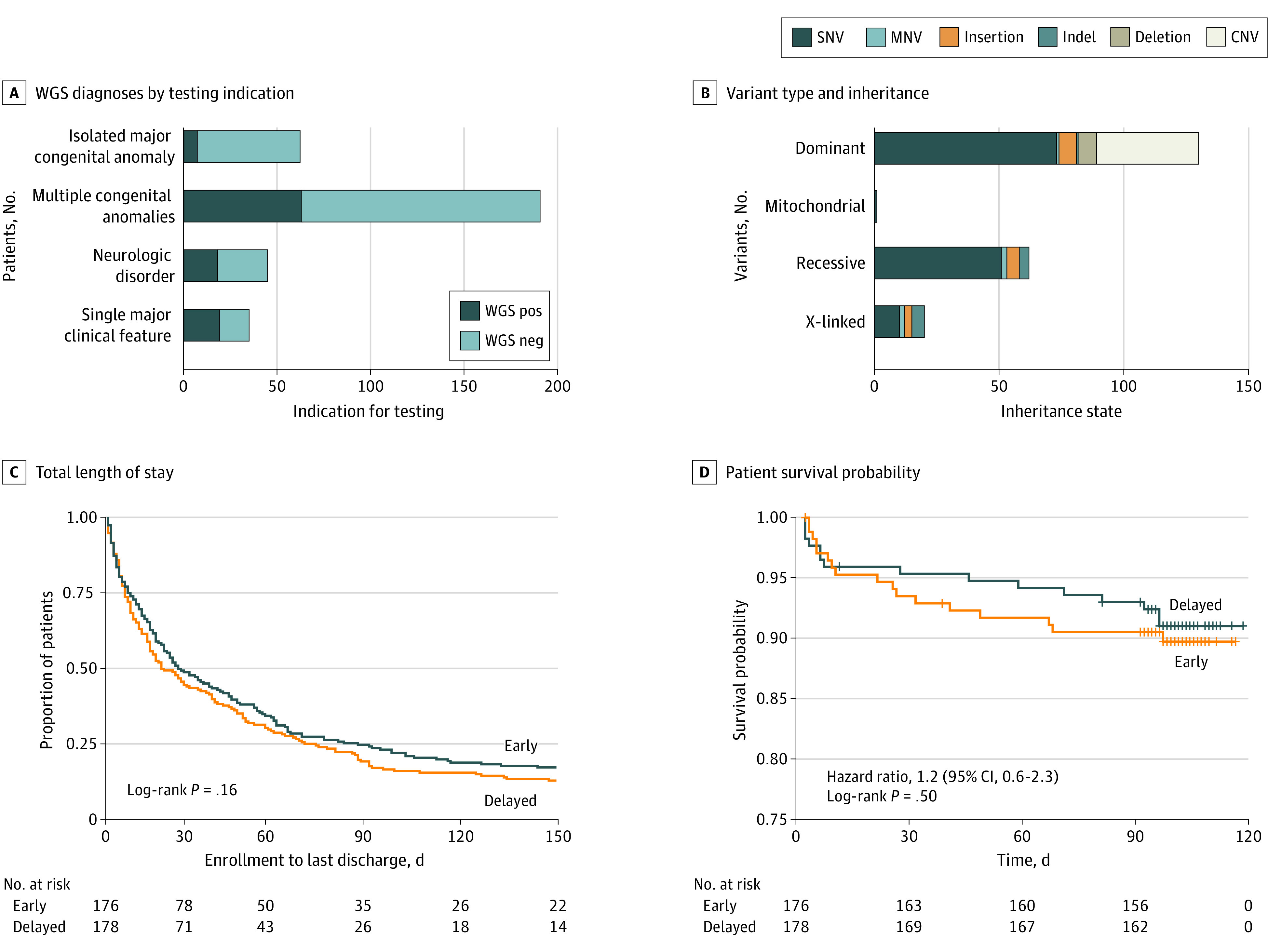
Main outcomes and measures: The main outcome was the difference in the proportion of infants in the early and delayed groups who received a change of management (COM) 60 days after enrollment. Additional outcome measures included WGS diagnostic efficacy, within-group COM at 90 days, length of hospital stay, and mortality.
Results: A total of 354 infants were randomized to the early (n = 176) or delayed (n = 178) arms. The mean participant age was 15 days (IQR, 7-32 days); 201 participants (56.8%) were boys; 19 (5.4%) were Asian; 47 (13.3%) were Black; 250 (70.6%) were White; and 38 (10.7%) were of other race. At 60 days, twice as many infants in the early group vs the delayed group received a COM (34 of 161 [21.1%; 95% CI, 15.1%-28.2%] vs 17 of 165 [10.3%; 95% CI, 6.1%-16.0%]; P = .009; odds ratio, 2.3; 95% CI, 1.22-4.32) and a molecular diagnosis (55 of 176 [31.0%; 95% CI, 24.5%-38.7%] vs 27 of 178 [15.0%; 95% CI, 10.2%-21.3%]; P < .001). At 90 days, the delayed group showed a doubling of COM (to 45 of 161 [28.0%; 95% CI, 21.2%-35.6%]) and diagnostic efficacy (to 56 of 178 [31.0%; 95% CI, 24.7%-38.8%]). The most frequent COMs across the observation window were subspecialty referrals (39 of 354; 11%), surgery or other invasive procedures (17 of 354; 4%), condition-specific medications (9 of 354; 2%), or other supportive alterations in medication (12 of 354; 3%). No differences in length of stay or survival were observed.
Conclusions and relevance: In this randomized clinical trial, for acutely ill infants in an intensive care unit, introduction of WGS was associated with a significant increase in focused clinical management compared with usual care. Access to first-line WGS may reduce health care disparities by enabling diagnostic equity. These data support WGS adoption and implementation in this population.
Trail registration: ClinicalTrials.gov Identifier: NCT03290469.
Conflict of interest statement
Figures
Comment in
-
Further Considerations on the Value of Whole-Genome Sequencing in Critically Ill Infants-Reply.JAMA Pediatr. 2022 Apr 1;176(4):422. doi: 10.1001/jamapediatrics.2021.6283. JAMA Pediatr. 2022. PMID: 35129608 No abstract available.
-
Further Considerations on the Value of Whole-Genome Sequencing in Critically Ill Infants.JAMA Pediatr. 2022 Apr 1;176(4):420-421. doi: 10.1001/jamapediatrics.2021.6280. JAMA Pediatr. 2022. PMID: 35129617 Free PMC article. No abstract available.
-
Further Considerations on the Value of Whole-Genome Sequencing in Critically Ill Infants.JAMA Pediatr. 2022 Apr 1;176(4):421-422. doi: 10.1001/jamapediatrics.2021.6286. JAMA Pediatr. 2022. PMID: 35129618 No abstract available.
References
-
- Dukhovny D, Zupancic JAF. Economic evaluation with clinical trials in neonatology. Neoreviews. 2011;12(2):e69-e75. doi: 10.1542/neo.12-2-e69 - DOI
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
