

Trends in Chronic Kidney Disease Care in the US by Race and Ethnicity, 2012-2019
- PMID: 34570204
- PMCID: PMC8477264
- DOI: 10.1001/jamanetworkopen.2021.27014
Trends in Chronic Kidney Disease Care in the US by Race and Ethnicity, 2012-2019
Abstract
Importance: Significant racial and ethnic disparities in chronic kidney disease (CKD) progression and outcomes are well documented, as is low use of guideline-recommended CKD care.
Objective: To examine guideline-recommended CKD care delivery by race and ethnicity in a large, diverse population.
Design, setting, and participants: In this serial cross-sectional study, adult patients with CKD that did not require dialysis, defined as a persistent estimated glomerular filtration rate less than 60 mL/min/1.73 m2 or a urine albumin-creatinine ratio of 30 mg/g or higher for at least 90 days, were identified in 2-year cross-sections from January 1, 2012, to December 31, 2019. Data from the OptumLabs Data Warehouse, a national data set of administrative and electronic health record data for commercially insured and Medicare Advantage patients, were used.
Exposures: The independent variables were race and ethnicity, as reported in linked electronic health records.
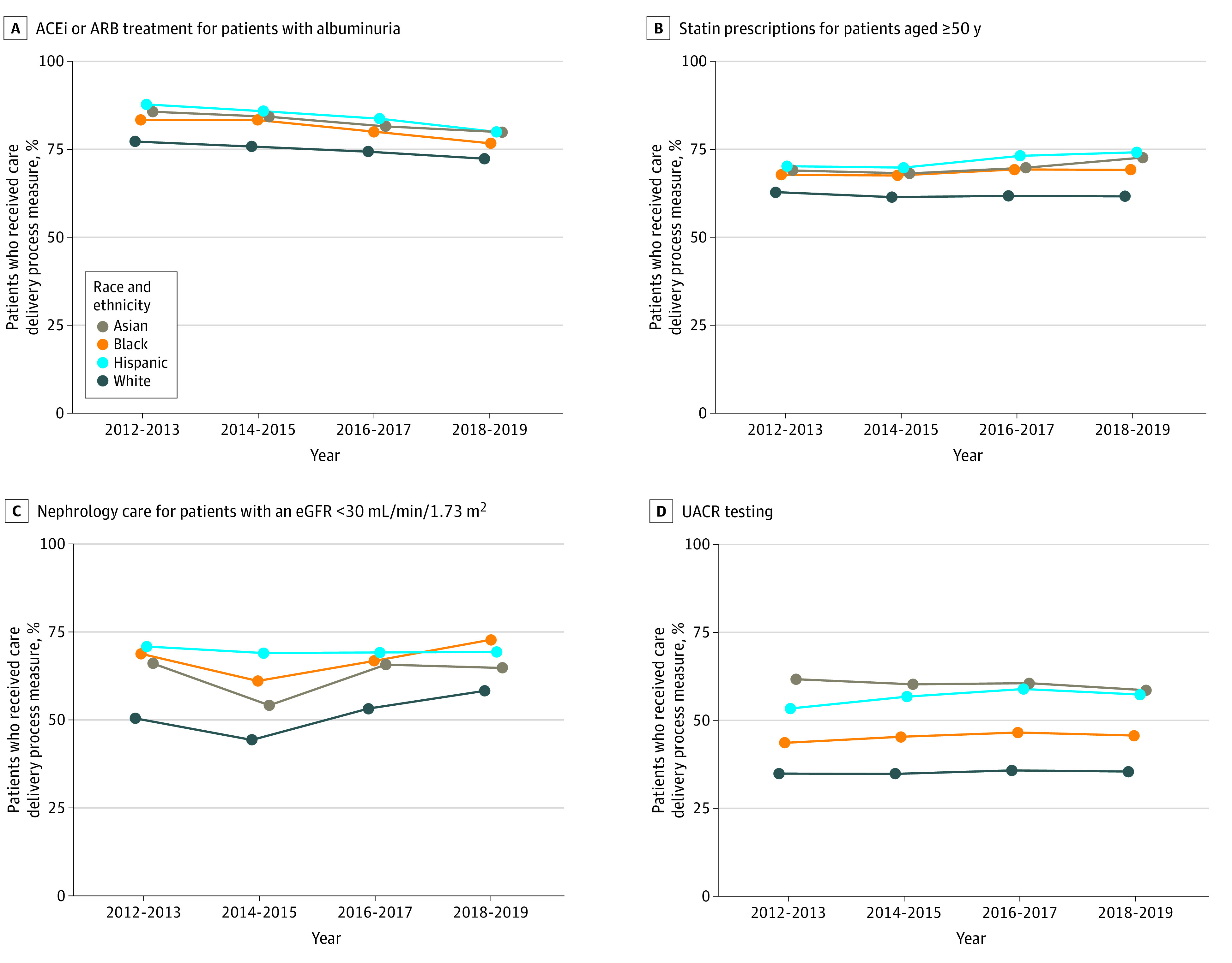
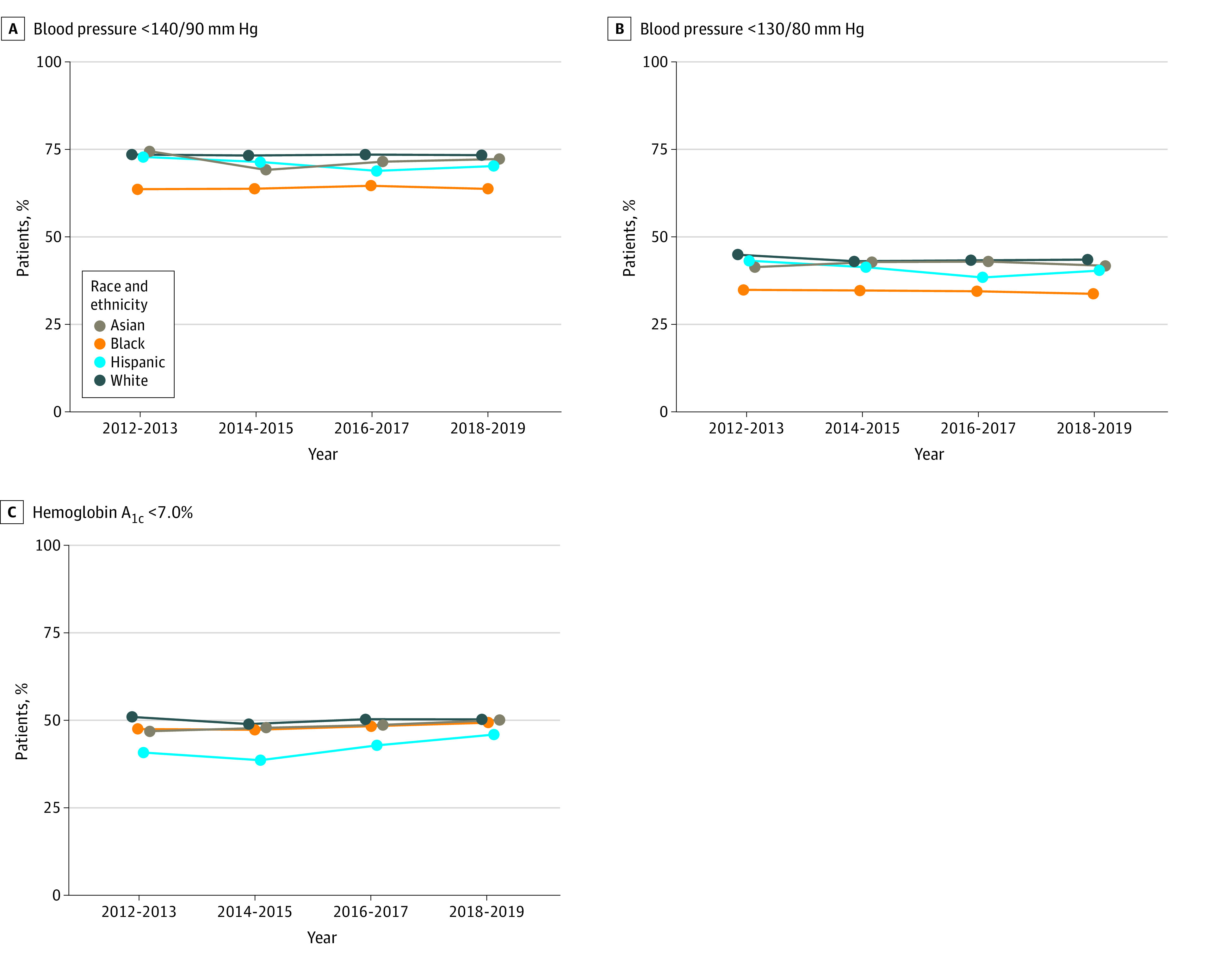
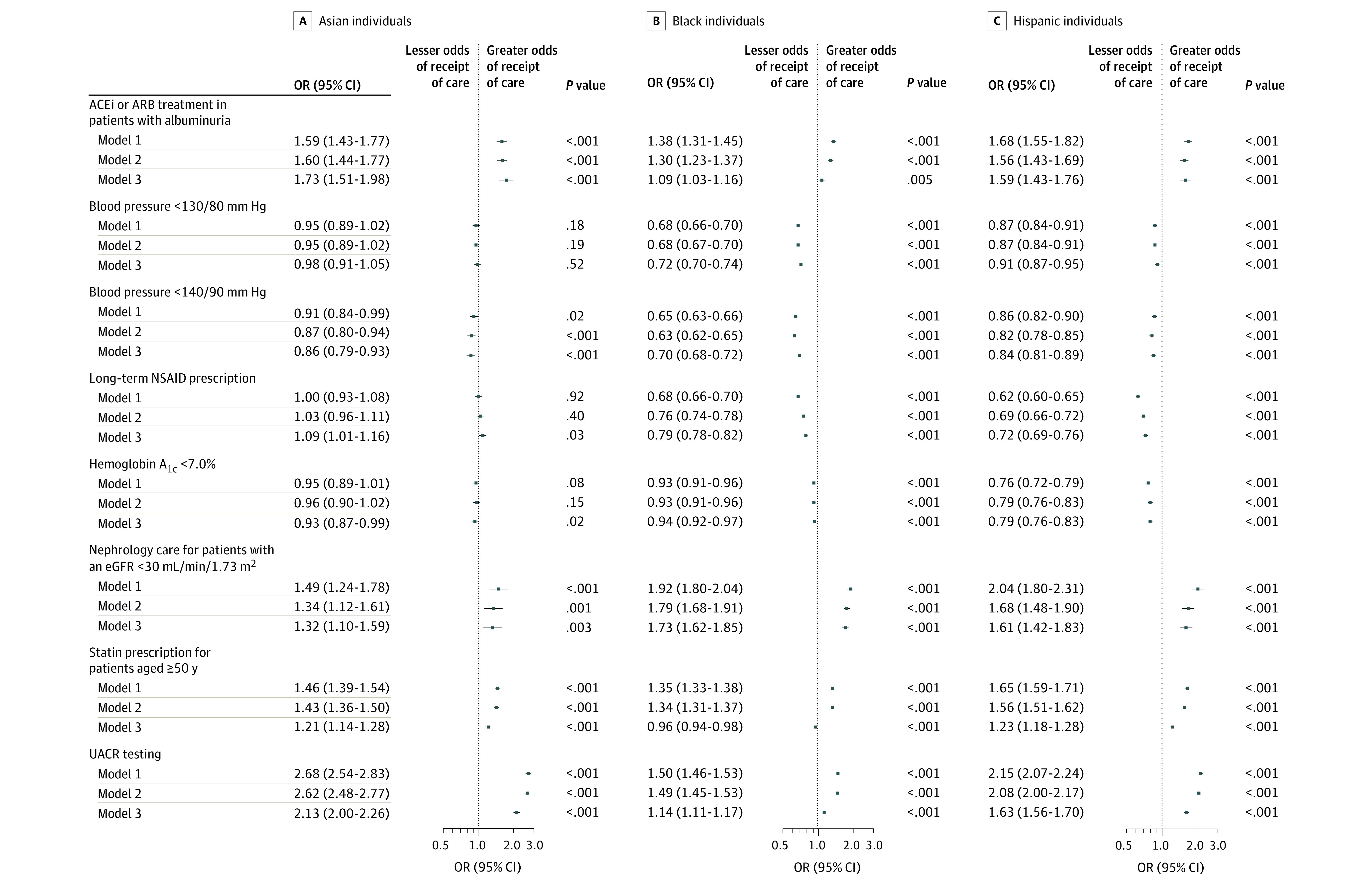
Main outcomes and measures: On the basis of guideline-recommended CKD care, the study examined care delivery process measures (angiotensin-converting enzyme inhibitor or angiotensin II receptor blocker prescription for albuminuria, statin prescription, albuminuria testing, nephrology care for CKD stage 4 or higher, and avoidance of chronic nonsteroidal anti-inflammatory drug prescription) and care delivery outcome measures (blood pressure and diabetes control).
Results: A total of 452 238 patients met the inclusion criteria (mean [SD] age, 74.0 [10.2] years; 262 089 [58.0%] female; a total of 7573 [1.7%] Asian, 49 970 [11.0%] Black, 15 540 [3.4%] Hispanic, and 379 155 [83.8%] White). Performance on process measures was higher among Asian, Black, and Hispanic patients compared with White patients for angiotensin-converting enzyme inhibitor and angiotensin II receptor blocker use (79.8% for Asian patients, 76.7% for Black patients, and 79.9% for Hispanic patients compared with 72.3% for White patients in 2018-2019), statin use (72.6% for Asian patients, 69.1% for Black patients, and 74.1% for Hispanic patients compared with 61.5% for White patients), nephrology care (64.8% for Asian patients, 72.9% for Black patients, and 69.4% for Hispanic patients compared with 58.3% for White patients), and albuminuria testing (53.9% for Asian patients, 41.0% for Black patients, and 52.6% for Hispanic patients compared with 30.7% for White patients). Achievement of blood pressure control to less than 140/90 mm Hg was similar or lower among Asian (71.8%), Black (63.3%), and Hispanic (69.8%) patients compared with White patients (72.9%). Achievement of diabetes control with hemoglobin A1c less than 7.0% was 50.1% in Asian patients, 49.3% in Black patients, and 46.0% in Hispanic patients compared with 50.3% for White patients.
Conclusions and relevance: Higher performance on CKD care process measures among Asian, Black, and Hispanic patients suggests that differences in medication prescription and diagnostic testing are unlikely to fully explain known disparities in CKD progression and kidney failure. Improving care delivery processes alone may be inadequate for reducing these disparities.
Conflict of interest statement
Figures
References
-
- United States Renal Data System . 2020 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2020.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
