

Impact of fetal trisomy 21 on umbilical artery Doppler indices
- PMID: 34570672
- PMCID: PMC10346994
- DOI: 10.1080/14767058.2021.1974388
Impact of fetal trisomy 21 on umbilical artery Doppler indices
Abstract
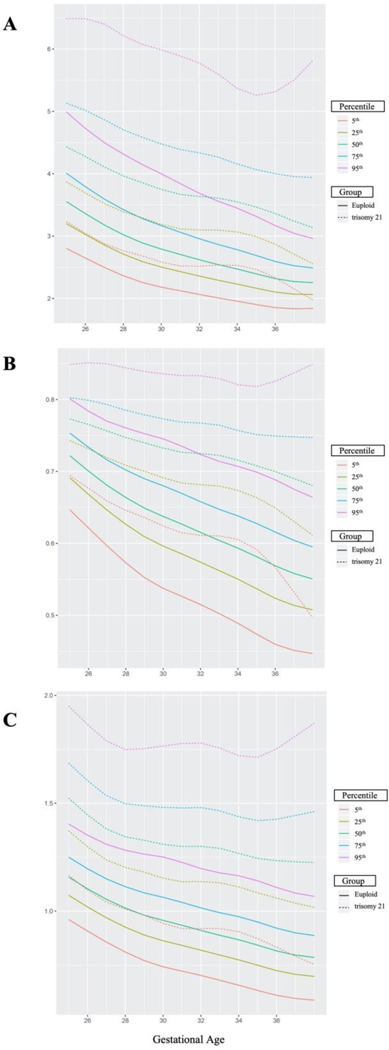
Objectives: Umbilical artery (UA) Doppler indices are surrogate measures of placental function, most commonly used to assess fetal wellbeing in pregnancies with fetal growth restriction. Fetuses with trisomy 21 (t21) are reported to have elevated UA Doppler indices, but reference percentiles are currently lacking for this population. We hypothesized that gestational age-specific values of UA Doppler indices in pregnancies complicated by t21 will be elevated compared to established percentiles based on euploid pregnancies. We aimed to assess UA Doppler indices longitudinally in fetuses with t21 in order to demonstrate Doppler patterns across gestation in this population, compare them with euploid fetuses, and investigate their association with pregnancy outcomes.
Methods: We conducted a retrospective cohort study of singleton pregnancies with confirmed fetal t21 who underwent UA Doppler surveillance antenatally from January 2012 to August 2019. UA Doppler indices, including systolic/diastolic (S/D) ratio, pulsatility index (PI), and resistance index (RI) were extracted from ultrasound reports or directly from ultrasound images. UA S/D, PI, and RI percentiles by gestational week were created from available observations from our cohort via a data-driven approach using a generalized additive model. A secondary analysis was run to statistically compare t21 values to established percentiles based on observations from a historical population of euploid fetuses.
Results: UA Doppler measurements from 86 t21 fetuses and 130 euploid fetuses were included in our analysis. Median (IQR) maternal age in t21 pregnancies and euploid pregnancies were 35 years (29-38) and 30 years (27-33), respectively. As in euploid fetuses, we found a negative association between Doppler indices and gestational age in the t21 fetuses. Maternal tobacco use, obesity, or chronic hypertension had no significant effect on UA Doppler indices. As hypothesized, values for UA S/D ratio, PI, and RI at the 2.5th, 5th, 10th, 25th, 50th, 75th, 90th, 95th, and 97.5th percentiles by gestational week were significantly higher in t21 fetuses compared to euploid fetuses (p<.001). Overall, 55.8% (48/86) of the t21 fetuses demonstrated at least one Doppler value above the 95th percentile for gestational age based on euploid reference standard. At birth, eight (9.3%) of the t21 fetuses were small for gestational age. When these pregnancies were removed from analysis, UA Doppler indices remained significantly higher than established percentiles at each week of gestation (p < .001). Only three pregnancies ended in fetal demise in the t21 population, two of which had persistently elevated Dopplers above the 95th percentile per established reference percentiles.
Conclusions: At each week of gestation, UA Doppler indices in t21 fetuses were significantly higher than established percentiles from a euploid population. Reference intervals based on euploid fetuses may therefore not be appropriate for antenatal surveillance of fetuses with t21. Prospective studies are needed to investigate the role and impact of serial UA Doppler velocimetry in the surveillance of pregnancies complicated by fetal t21.
Keywords: Doppler index; aneuploidy; trisomy 21; ultrasound; umbilical artery.
Conflict of interest statement
The authors report no conflict of interest.
Figures
Similar articles
-
Umbilical artery pulsatility index and half-peak systolic velocity deceleration time in fetuses with trisomy 21.J Matern Fetal Neonatal Med. 2020 Oct;33(20):3469-3475. doi: 10.1080/14767058.2019.1575357. Epub 2019 Feb 10. J Matern Fetal Neonatal Med. 2020. PMID: 30741044
-
Clinical impact of Doppler reference charts on management of small-for-gestational-age fetuses: need for standardization.Ultrasound Obstet Gynecol. 2020 Aug;56(2):166-172. doi: 10.1002/uog.20380. Epub 2020 Jun 30. Ultrasound Obstet Gynecol. 2020. PMID: 31237023
-
Sex differences in umbilical artery Doppler indices: a longitudinal study.Biol Sex Differ. 2018 Apr 18;9(1):16. doi: 10.1186/s13293-018-0174-x. Biol Sex Differ. 2018. PMID: 29669590 Free PMC article.
-
Umbilical and fetal middle cerebral artery Doppler reference ranges in a twin population followed longitudinally from 24 to 38 weeks' gestation.Ultrasound Obstet Gynecol. 2014 Oct;44(4):461-7. doi: 10.1002/uog.13302. Epub 2014 Sep 5. Ultrasound Obstet Gynecol. 2014. PMID: 24407772
-
Clinical Opinion: The diagnosis and management of suspected fetal growth restriction: an evidence-based approach.Am J Obstet Gynecol. 2022 Mar;226(3):366-378. doi: 10.1016/j.ajog.2021.11.1357. Epub 2022 Jan 10. Am J Obstet Gynecol. 2022. PMID: 35026129 Free PMC article. Review.
Cited by
-
Case Report: Two cases of apparent discordance between non-invasive prenatal testing (NIPT) and amniocentesis resulting in feto-placental mosaicism of trisomy 21. Issues in diagnosis, investigation and counselling.Front Genet. 2022 Oct 25;13:982508. doi: 10.3389/fgene.2022.982508. eCollection 2022. Front Genet. 2022. PMID: 36386832 Free PMC article.
References
-
- Alfirevic Z, Neilson JP. Doppler ultrasonography in high-risk pregnancies: systematic review with meta-analysis. Am J Obstet Gynecol. 1995; 172: 1379–1387. - PubMed
-
- Acharya G, Wilsgaard T, Berntsen GK, et al. Reference ranges for serial measurements of umbilical artery Doppler indices in the second half of pregnancy. Am J Obstet Gynecol. 2005; 192: 937–944. - PubMed
-
- Martinez Crespo JM, Comas C, Ojuel H, et al.. Fortuny A. Umbilical artery pulsatility index in early pregnancies with chromosome anomalies. Br J Obstet Gynaecol. 1996; 103: 330–334. - PubMed
-
- Martinez JM, Borrell A, Antolin E, et al. Combining nuchal translucency with umbilical Doppler velocimetry for detecting fetal trisomies in the first trimester of pregnancy. Br J Obstet Gynaecol. 1997; 104: 11–14. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous