

Pilot Study of Anti-Th2 Immunotherapy for the Treatment of Breast Cancer-Related Upper Extremity Lymphedema
- PMID: 34571811
- PMCID: PMC8466465
- DOI: 10.3390/biology10090934
Pilot Study of Anti-Th2 Immunotherapy for the Treatment of Breast Cancer-Related Upper Extremity Lymphedema
Abstract
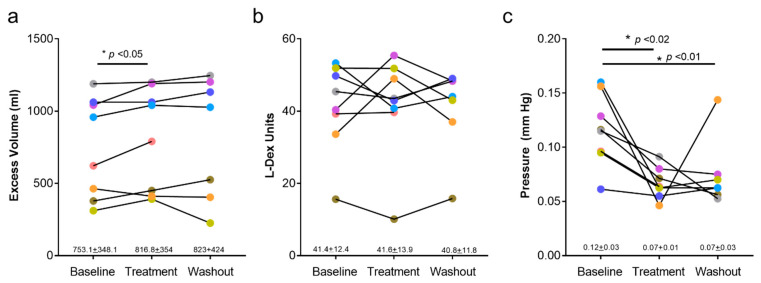
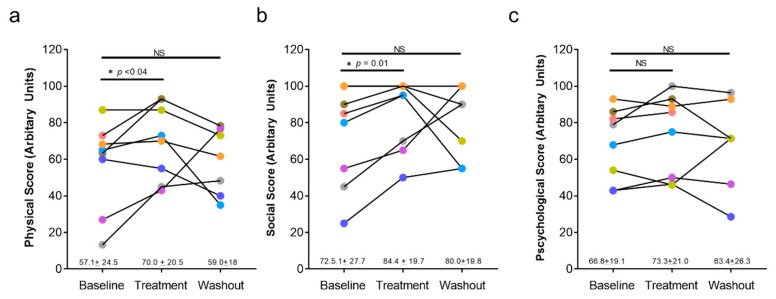
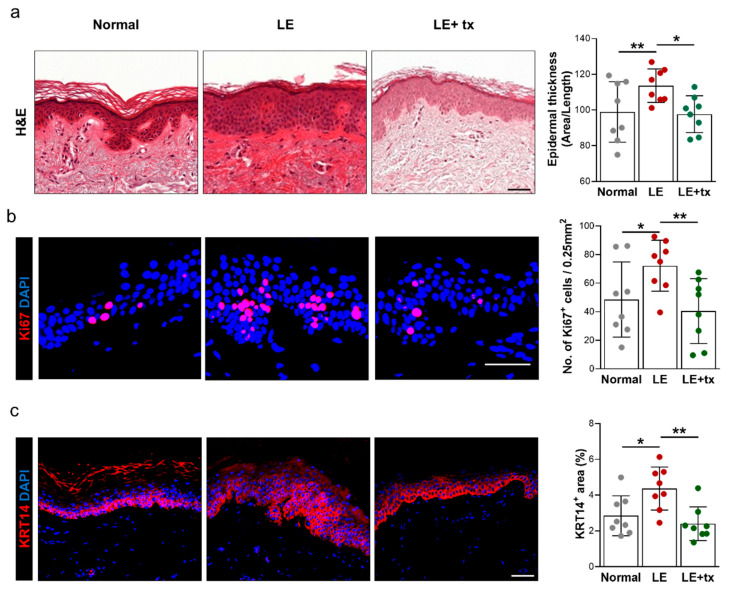
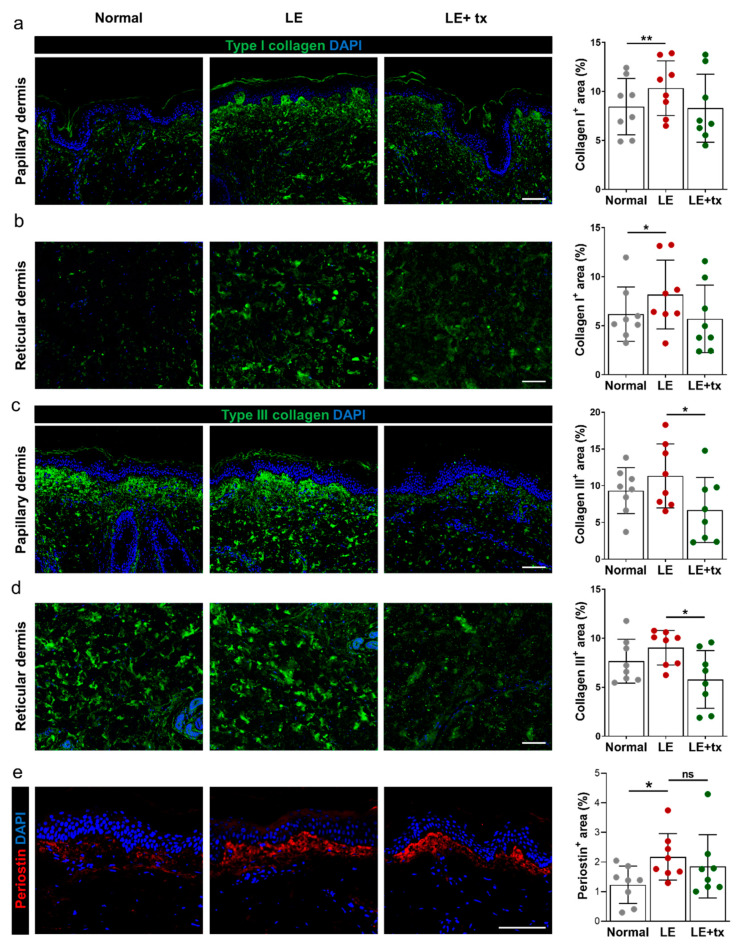
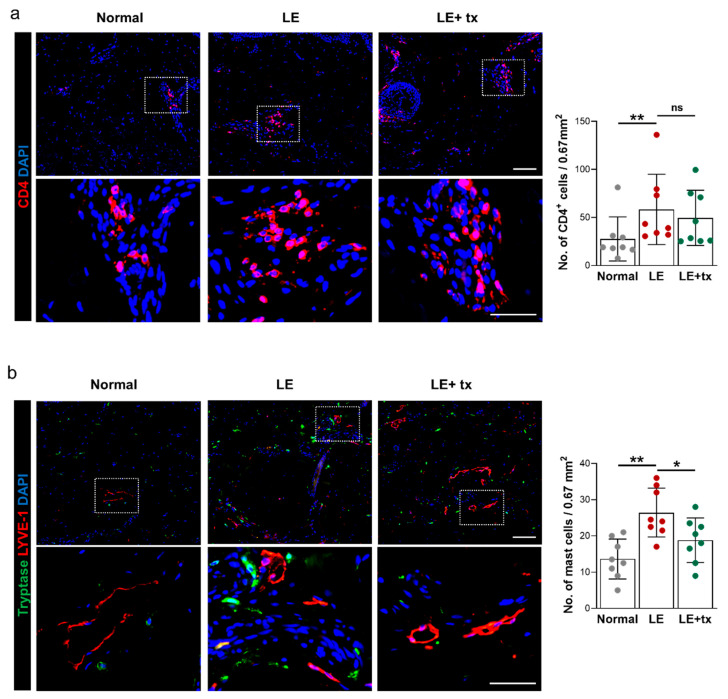
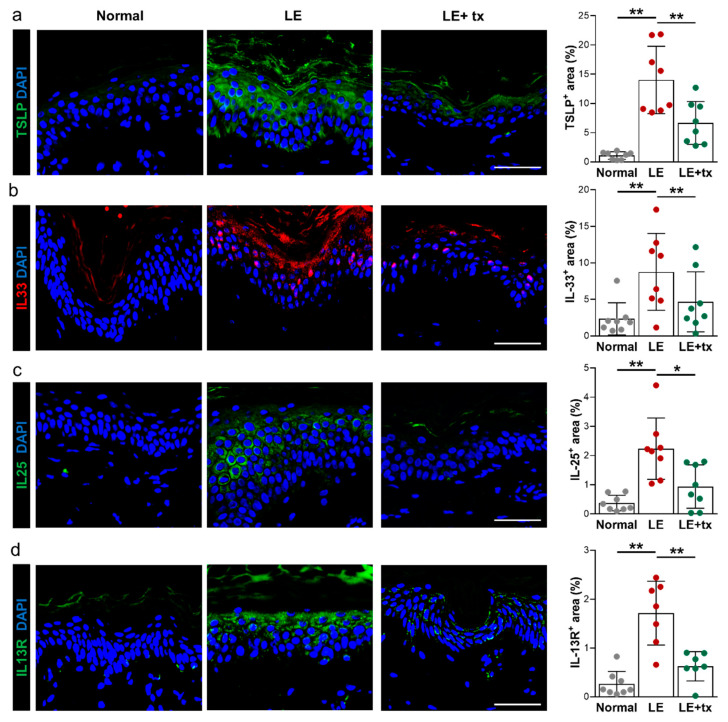
Recent studies suggest that Th2 cells play a key role in the pathology of secondary lymphedema by elaborating cytokines such as IL4 and IL13. The aim of this study was to test the efficacy of QBX258, a monoclonal IL4/IL13 neutralizing antibody, in women with breast cancer-related lymphedema (BCRL). We enrolled nine women with unilateral stage I/II BCRL and treated them once monthly with intravenous infusions of QBX258 for 4 months. We measured limb volumes, bioimpedance, and skin tonometry, and analyzed the quality of life (QOL) using a validated lymphedema questionnaire (Upper Limb Lymphedema 27, ULL-27) before treatment, immediately after treatment, and 4 months following treatment withdrawal. We also obtained 5 mm skin biopsies from the normal and lymphedematous limbs before and after treatment. Treatment was well-tolerated; however, one patient with a history of cellulitis developed cellulitis during the trial and was excluded from further analysis. We found no differences in limb volumes or bioimpedance measurements after drug treatment. However, QBX258 treatment improved skin stiffness (p < 0.001) and improved QOL measurements (Physical p < 0.05, Social p = 0.01). These improvements returned to baseline after treatment withdrawal. Histologically, treatment decreased epidermal thickness, the number of proliferating keratinocytes, type III collagen deposition, infiltration of mast cells, and the expression of Th2-inducing cytokines in the lymphedematous skin. Our limited study suggests that immunotherapy against Th2 cytokines may improve skin changes and QOL of women with BCRL. This treatment appears to be less effective for decreasing limb volumes; however, additional studies are needed.
Keywords: Th2 inflammation; breast cancer; immunotherapy; keratinocytes; lymphedema; skin.
Conflict of interest statement
Babak J. Mehrara is an advisor to PureTech Corp. Joseph H. Dayan is a paid advisor to Stryker Corp.
Figures
References
-
- McLaughlin S.A., Wright M.J., Morris K.T., Giron G.L., Sampson M.R., Brockway J.P., Hurley K.E., Riedel E.R., Van Zee K.J. Prevalence of lymphedema in women with breast cancer 5 years after sentinel lymph node biopsy or axillary dissection: Objective measurements. J. Clin. Oncol. 2008;26:5213–5219. doi: 10.1200/JCO.2008.16.3725. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
