

Oncologic Imaging of the Lymphatic System: Current Perspective with Multi-Modality Imaging and New Horizon
- PMID: 34572781
- PMCID: PMC8465736
- DOI: 10.3390/cancers13184554
Oncologic Imaging of the Lymphatic System: Current Perspective with Multi-Modality Imaging and New Horizon
Abstract
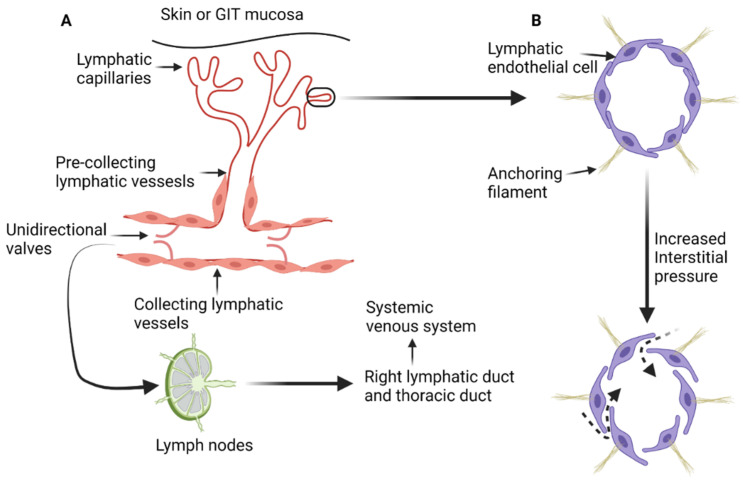
The lymphatic system is an anatomically complex vascular network that is responsible for interstitial fluid homeostasis, transport of large interstitial particles and cells, immunity, and lipid absorption in the gastrointestinal tract. This network of specially adapted vessels and lymphoid tissue provides a major pathway for metastatic spread. Many malignancies produce vascular endothelial factors that induce tumoral and peritumoral lymphangiogenesis, increasing the likelihood for lymphatic spread. Radiologic evaluation for disease staging is the cornerstone of oncologic patient treatment and management. Multiple imaging modalities are available to access both local and distant metastasis. In this manuscript, we review the anatomy, physiology, and imaging of the lymphatic system.
Keywords: conventional lymphography; lymphangiography; lymphatic metastasis; lymphatic system anatomy; lymphatic system imaging; lymphatic system physiology; lymphoscintigraphy; magnetic resonance lymphangiography.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Novel Lymphatic Imaging Techniques.Tech Vasc Interv Radiol. 2016 Dec;19(4):255-261. doi: 10.1053/j.tvir.2016.10.002. Epub 2016 Oct 6. Tech Vasc Interv Radiol. 2016. PMID: 27993320 Review.
-
Lack of functioning lymphatics and accumulation of tissue fluid/lymph in interstitial "lakes" in colon cancer tissue.Lymphology. 2010 Dec;43(4):158-67. Lymphology. 2010. PMID: 21446571
-
Magnetic resonance imaging versus lymphoscintigraphy for the assessment of focal lymphatic transport disorders of the lower limb: first experiences.Nuklearmedizin. 2014;53(5):190-6. doi: 10.3413/Nukmed-0649-14-03. Epub 2014 Jul 7. Nuklearmedizin. 2014. PMID: 24999013
-
Posttraumatic edema of the lower extremities: evaluation of the lymphatic vessels with magnetic resonance lymphangiography.J Vasc Surg. 2009 Feb;49(2):417-23. doi: 10.1016/j.jvs.2008.08.069. J Vasc Surg. 2009. PMID: 19216961
-
Lymphatic Anatomy.Tech Vasc Interv Radiol. 2016 Dec;19(4):247-254. doi: 10.1053/j.tvir.2016.10.003. Epub 2016 Oct 8. Tech Vasc Interv Radiol. 2016. PMID: 27993319 Review.
Cited by
-
Impact of Ascending HPV Infection on Colorectal Cancer Risk: Evidence from a Nationwide Study.Microorganisms. 2024 Aug 23;12(9):1746. doi: 10.3390/microorganisms12091746. Microorganisms. 2024. PMID: 39338421 Free PMC article.
-
In Vitro, In Vivo, and In Silico Models of Lymphangiogenesis in Solid Malignancies.Cancers (Basel). 2022 Mar 16;14(6):1525. doi: 10.3390/cancers14061525. Cancers (Basel). 2022. PMID: 35326676 Free PMC article. Review.
References
-
- Al-Kofahi M., Yun J.W., Minagar A., Alexander J.S. Anatomy and roles of lymphatics in inflammatory diseases. Clin. Exp. Neuroimmunol. 2017;8:199–214. doi: 10.1111/cen3.12400. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Medical
