

Inflammatory Biomarker Score Identifies Patients with Six-Fold Increased Risk of One-Year Mortality after Pancreatic Cancer
- PMID: 34572824
- PMCID: PMC8466571
- DOI: 10.3390/cancers13184599
Inflammatory Biomarker Score Identifies Patients with Six-Fold Increased Risk of One-Year Mortality after Pancreatic Cancer
Abstract
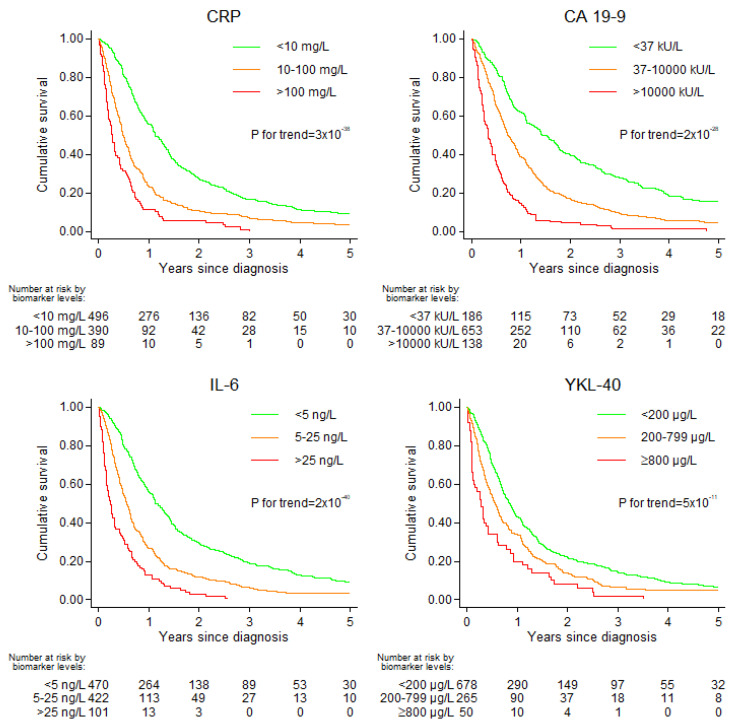
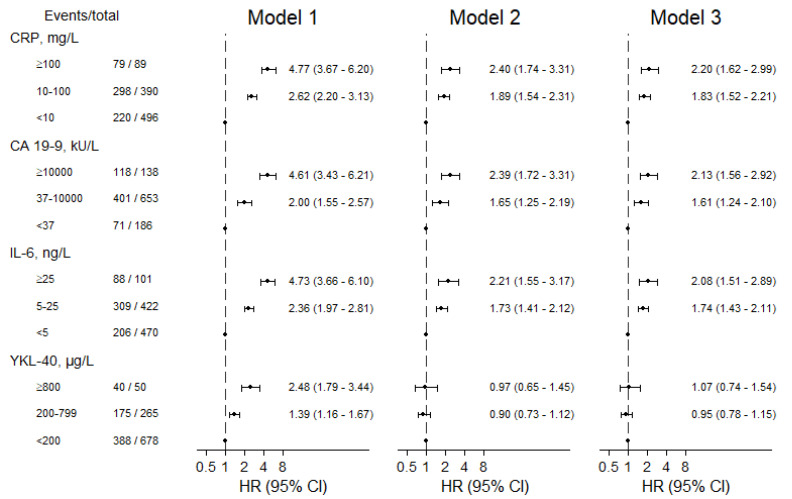
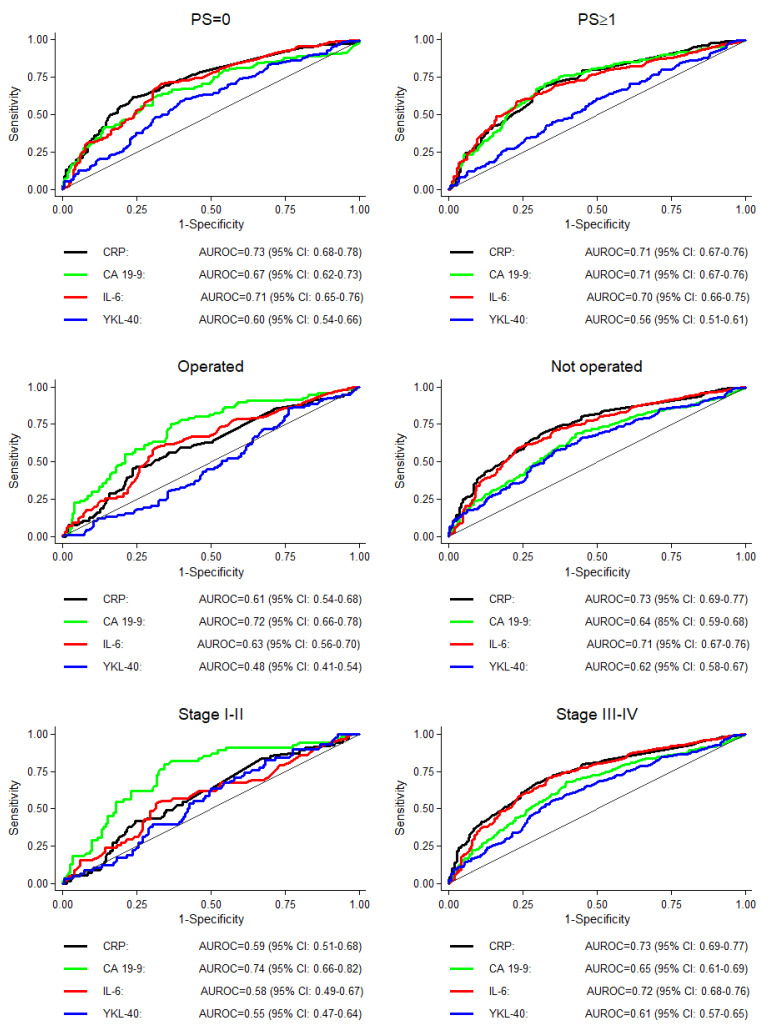
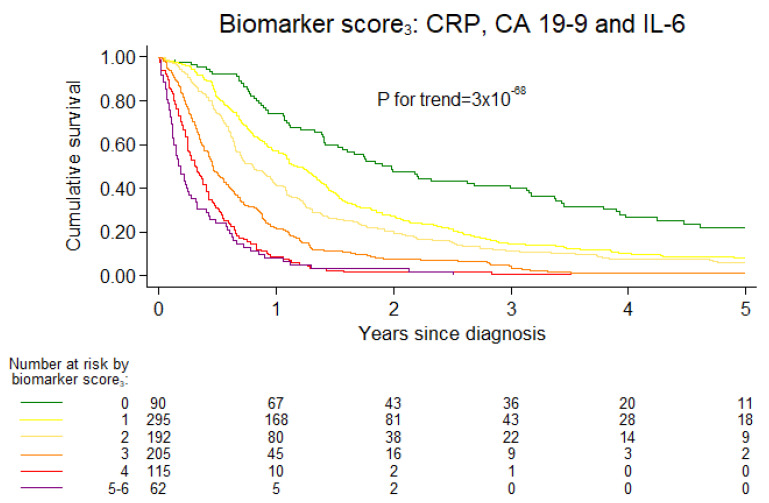
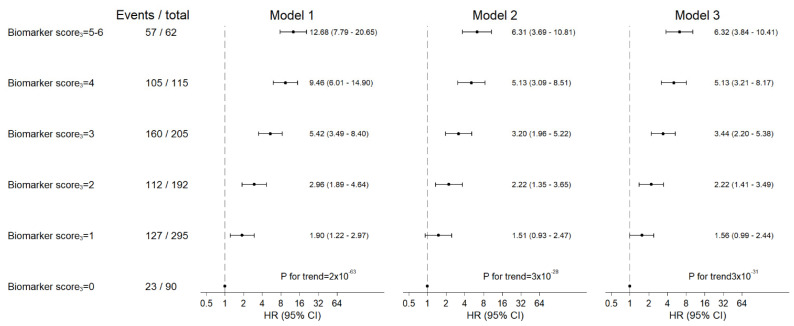
We examined whether elevated plasma C-reactive protein (CRP), carbohydrate antigen (CA) 19-9, interleukin-6 (IL-6) and YKL-40, individually or combined, can identify poor survivors among patients with pancreatic ductal adenocarcinoma (PDAC). We measured CRP, CA 19-9, IL-6 and YKL-40 in 993 patients at the time of PDAC diagnosis. The biomarker score was the sum of biomarker categories, coded 0, 1 and 2 for low, intermediate and high plasma concentrations, respectively. High vs. low levels of CRP, CA 19-9 and IL-6 were each independently associated with a two-fold increased risk of one-year mortality. CRP performed best in patients with advanced and CA 19-9 in patients with low cancer stages. YKL-40 was not associated with mortality and, therefore, was not included in the biomarker score. Compared to the biomarker score = 0, the multifactorially adjusted hazard ratios for one-year mortality were 1.56 (95% confidence interval: 0.99-2.44) for score = 1, 2.22 (1.41-3.49) for score = 2, 3.44 (2.20-5.38) for score = 3, 5.13 (3.21-8.17) for score = 4 and 6.32 (3.84-10.41) for score = 5-6 (p-value for trend = 3 × 10-31). This score performed better than any single biomarker or combination of biomarkers when examined in similarly sized or other categories. In conclusion, a combination score of elevated CRP, CA 19-9 and IL-6 identified patients with six-fold higher one-year mortality.
Keywords: C-reactive protein; CA-19-9 antigen; carcinoma; chitinase-3-like protein 1; interleukin-6; pancreatic ductal.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
