

Selective Serotonin Reuptake Inhibitors for the Treatment of Depression in Adults with Down Syndrome: A Preliminary Retrospective Chart Review Study
- PMID: 34573236
- PMCID: PMC8469816
- DOI: 10.3390/brainsci11091216
Selective Serotonin Reuptake Inhibitors for the Treatment of Depression in Adults with Down Syndrome: A Preliminary Retrospective Chart Review Study
Abstract
Background: Depression is a common psychiatric comorbidity in individuals with Down syndrome (DS), particularly adults, with an estimated lifetime prevalence of at least 10%. The current literature on the treatment of depression in adults with DS is limited to case series published more than two decades ago, prior to the widespread use of modern antidepressant medications such as selective serotonin reuptake inhibitors (SSRIs). The purpose of this retrospective chart review study was to examine the effectiveness, tolerability, and safety of SSRIs for depression in adults with DS.
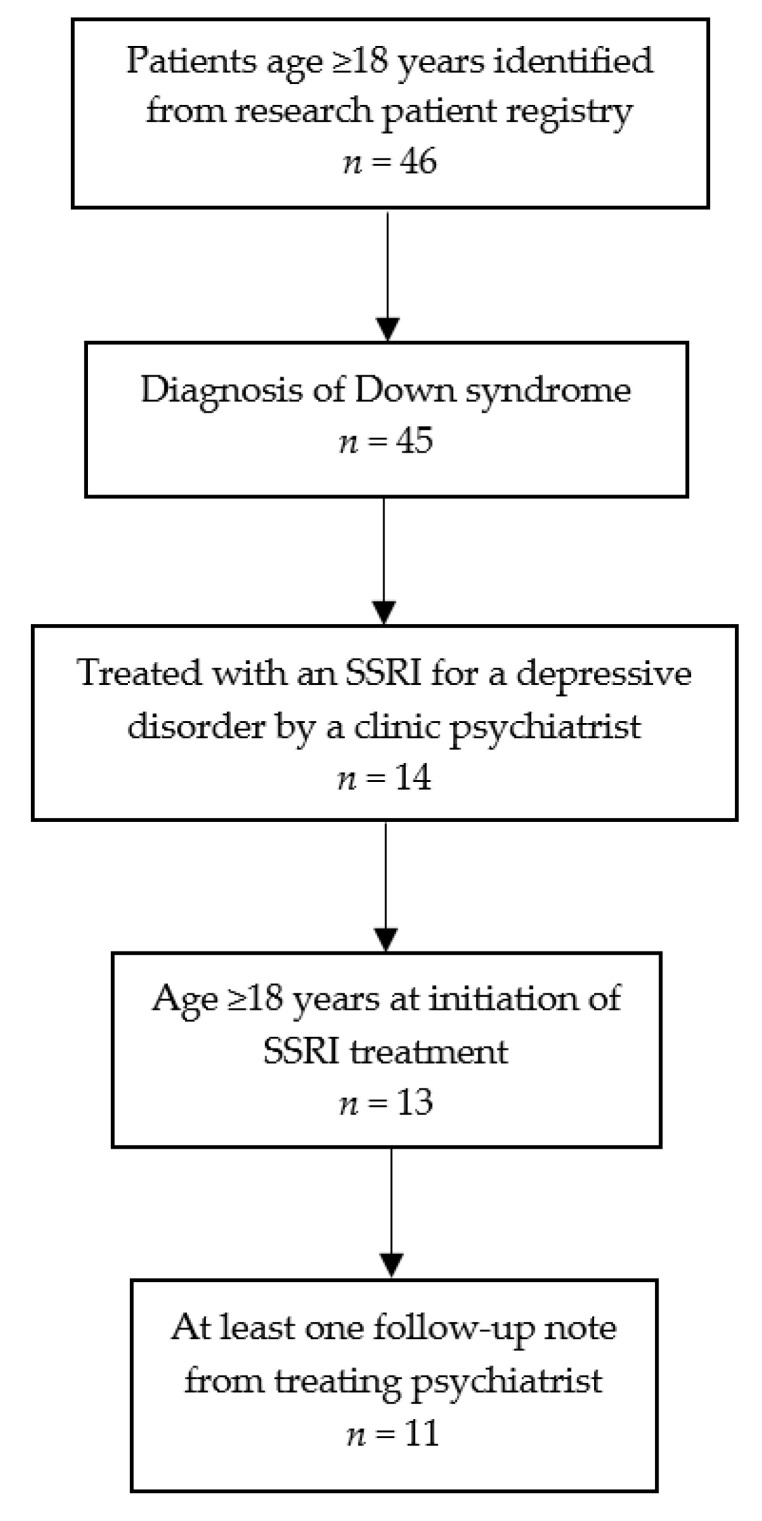
Methods: Medical records of 11 adults with DS and depression were reviewed. Assignment of scores for severity (S) of symptoms of depression and improvement (I) of symptoms with treatment with an SSRI was made retrospectively using the Clinical Global Impression Scale (CGI). Demographic and clinical characteristics of the study population, SSRI name, dose, and duration of treatment; and adverse effects were also recorded.
Results: All 11 patients (7 male, 4 female; mean age = 27.2 years, range 18-46 years) completed a 12-week treatment course with an SSRI. The median duration of time after initiation of the SSRI covered by record review was 2.1 years, with a range of 24 weeks to 6.7 years. Nine of the 11 patients (82%; 95% CI 52%, 95%) were judged responders to SSRIs based on a rating of "much improved" or "very much improved" on the CGI-I after 12 weeks of treatment (median time of follow-up was 14.4 weeks, with a range of 12.0-33.0 weeks). Adverse effects occurred in four patients (36%). The most common adverse effects were daytime sedation and anger.
Conclusions: In this preliminary retrospective study, the majority of patients responded to a 12-week course of SSRI treatment and some tolerated long-term use. Controlled studies are needed to further assess the efficacy, tolerability, and safety of SSRIs for the treatment of depression in adults with DS.
Keywords: Down syndrome; depression; selective serotonin reuptake inhibitor.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- CDC Facts about Down Syndrome. [(accessed on 25 June 2020)]; Available online: https://www.cdc.gov/ncbddd/birthdefects/downsyndrome.html.
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
