

Hemodynamic Monitoring in Sepsis-A Conceptual Framework of Macro- and Microcirculatory Alterations
- PMID: 34573901
- PMCID: PMC8469937
- DOI: 10.3390/diagnostics11091559
Hemodynamic Monitoring in Sepsis-A Conceptual Framework of Macro- and Microcirculatory Alterations
Abstract
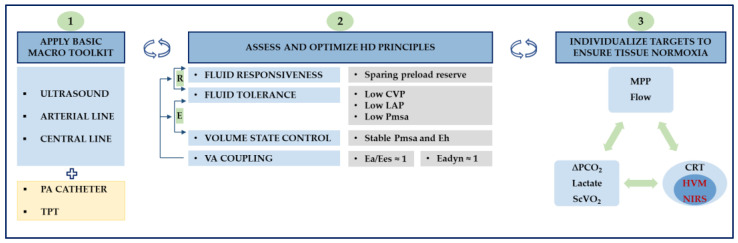
Circulatory failure in sepsis is common and places a considerable burden on healthcare systems. It is associated with an increased likelihood of mortality, and timely recognition is a prerequisite to ensure optimum results. While there is consensus that aggressive source control, adequate antimicrobial therapy and hemodynamic management constitute crucial determinants of outcome, discussion remains about the best way to achieve each of these core principles. Sound cardiovascular support rests on tailored fluid resuscitation and vasopressor therapy. To this end, an overarching framework to improve cardiovascular dynamics has been a recurring theme in modern critical care. The object of this review is to examine the nature of one such framework that acknowledges the growing importance of adaptive hemodynamic support combining macro- and microhemodynamic variables to produce adequate tissue perfusion.
Keywords: hemodynamic; macrocirculation; microcirculation; monitoring; sepsis; shock.
Conflict of interest statement
The authors declare no conflict of interest.
Figures





References
-
- Rhodes A., Evans L., Alhazanni W., Levy M., Antonelli M., Ferrer R., Kumar A., Sevransky J., Sprung C.L., Nunnally M.E., et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Crit. Care Med. 2017;45:486–552. doi: 10.1097/CCM.0000000000002255. - DOI - PubMed
-
- Singer M., Deutschman C.S., Seymour C.C., Shankar-Hari M., Annane D., Bauer M., Bellomo R., Bernard G.R., Chiche J.-D., Coopersmith C.C., et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) JAMA. 2016;315:801–810. doi: 10.1001/jama.2016.0287. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
