

CT-Based Risk Stratification for Intensive Care Need and Survival in COVID-19 Patients-A Simple Solution
- PMID: 34573957
- PMCID: PMC8465083
- DOI: 10.3390/diagnostics11091616
CT-Based Risk Stratification for Intensive Care Need and Survival in COVID-19 Patients-A Simple Solution
Abstract
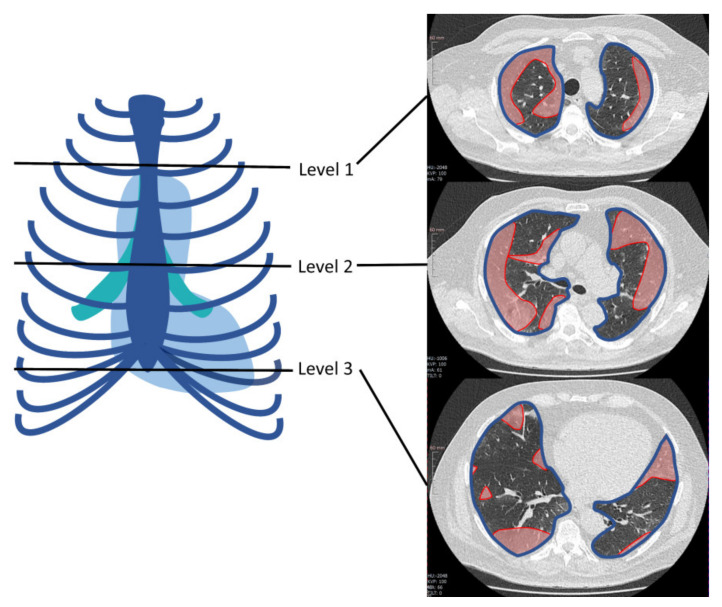
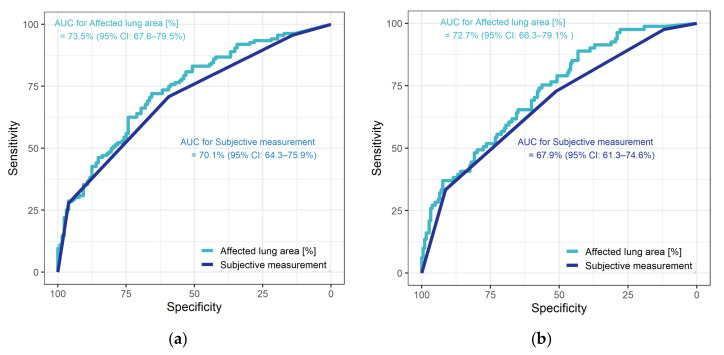
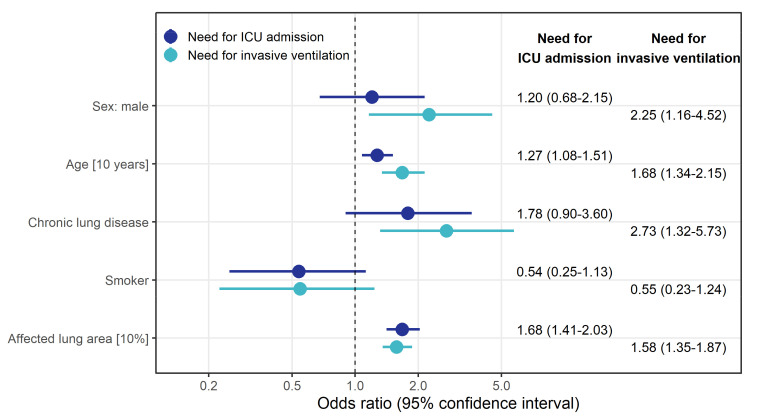
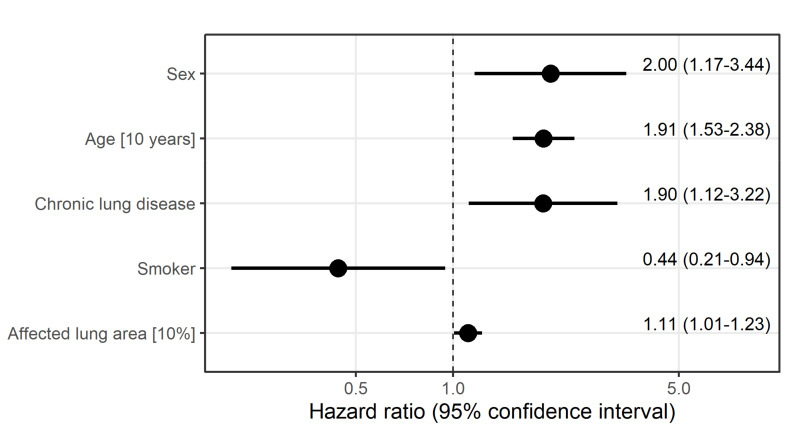
We evaluated a simple semi-quantitative (SSQ) method for determining pulmonary involvement in computed tomography (CT) scans of COVID-19 patients. The extent of lung involvement in the first available CT was assessed with the SSQ method and subjectively. We identified risk factors for the need of invasive ventilation, intensive care unit (ICU) admission and for time to death after infection. Additionally, the diagnostic performance of both methods was evaluated. With the SSQ method, a 10% increase in the affected lung area was found to significantly increase the risk for need of ICU treatment with an odds ratio (OR) of 1.68 and for invasive ventilation with an OR of 1.35. Male sex, age, and pre-existing chronic lung disease were also associated with higher risks. A larger affected lung area was associated with a higher instantaneous risk of dying (hazard ratio (HR) of 1.11) independently of other risk factors. SSQ measurement was slightly superior to the subjective approach with an AUC of 73.5% for need of ICU treatment and 72.7% for invasive ventilation. SSQ assessment of the affected lung in the first available CT scans of COVID-19 patients may support early identification of those with higher risks for need of ICU treatment, invasive ventilation, or death.
Keywords: COVID-19; CT; SARS-CoV-2; developing countries; intensive care; quantification; resource allocation; risk assessment.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Diagnostic Value of Initial Chest CT Findings for the Need of ICU Treatment/Intubation in Patients with COVID-19.Diagnostics (Basel). 2020 Nov 10;10(11):929. doi: 10.3390/diagnostics10110929. Diagnostics (Basel). 2020. PMID: 33182695 Free PMC article.
-
Artificial intelligence (AI)-assisted chest computer tomography (CT) insights: a study on intensive care unit (ICU) admittance trends in 78 coronavirus disease 2019 (COVID-19) patients.J Thorac Dis. 2024 Feb 29;16(2):1009-1020. doi: 10.21037/jtd-23-1150. Epub 2024 Feb 26. J Thorac Dis. 2024. PMID: 38505008 Free PMC article.
-
Cohort of Four Thousand Four Hundred Four Persons Under Investigation for COVID-19 in a New York Hospital and Predictors of ICU Care and Ventilation.Ann Emerg Med. 2020 Oct;76(4):394-404. doi: 10.1016/j.annemergmed.2020.05.011. Epub 2020 May 11. Ann Emerg Med. 2020. PMID: 32563601 Free PMC article.
-
CT-derived Chest Muscle Metrics for Outcome Prediction in Patients with COVID-19.Radiology. 2021 Aug;300(2):E328-E336. doi: 10.1148/radiol.2021204141. Epub 2021 Mar 16. Radiology. 2021. PMID: 33724065 Free PMC article.
-
Risk factors for invasive aspergillosis in ICU patients with COVID-19: current insights and new key elements.Ann Intensive Care. 2021 Sep 15;11(1):136. doi: 10.1186/s13613-021-00923-4. Ann Intensive Care. 2021. PMID: 34524562 Free PMC article. Review.
Cited by
-
Prognostic findings for ICU admission in patients with COVID-19 pneumonia: baseline and follow-up chest CT and the added value of artificial intelligence.Emerg Radiol. 2022 Apr;29(2):243-262. doi: 10.1007/s10140-021-02008-y. Epub 2022 Jan 20. Emerg Radiol. 2022. PMID: 35048222 Free PMC article. Review.
-
Analysis of Deaths and Favorable Developments of Patients with SARS-CoV-2 Hospitalized in the Largest Hospital for Infectious Diseases and Pneumo-Phthisiology in the West of the Country.Int J Gen Med. 2022 Mar 29;15:3417-3431. doi: 10.2147/IJGM.S359483. eCollection 2022. Int J Gen Med. 2022. PMID: 35378919 Free PMC article.
References
-
- W.W.H. Organization WHO Coronavirus (COVID-19) Dashboard. WHO Health Emergency Dashboard. 2020. [(accessed on 5 May 2021)]. Available online: https://covid19.who.int/
-
- Rodriguez-Morales A.J., Cardona-Ospina J.A., Gutiérrez-Ocampo E., Villamizar-Peña R., Holguin-Rivera Y., Escalera-Antezana J.P., Alvarado-Arnez L.E., Bonilla-Aldana D.K., Franco-Paredes C., Henao-Martinez A.F., et al. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2020;34:101623. doi: 10.1016/j.tmaid.2020.101623. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
