

Understanding the Role of External Facilitation to Drive Quality Improvement for Stroke Care in Hospitals
- PMID: 34574869
- PMCID: PMC8471416
- DOI: 10.3390/healthcare9091095
Understanding the Role of External Facilitation to Drive Quality Improvement for Stroke Care in Hospitals
Abstract
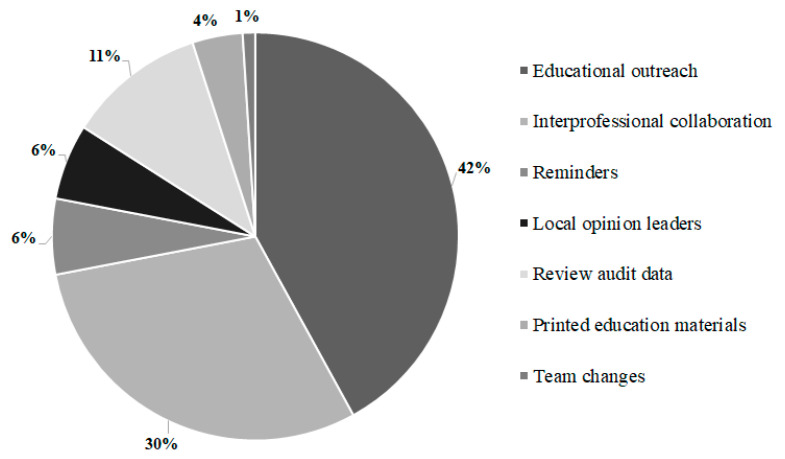
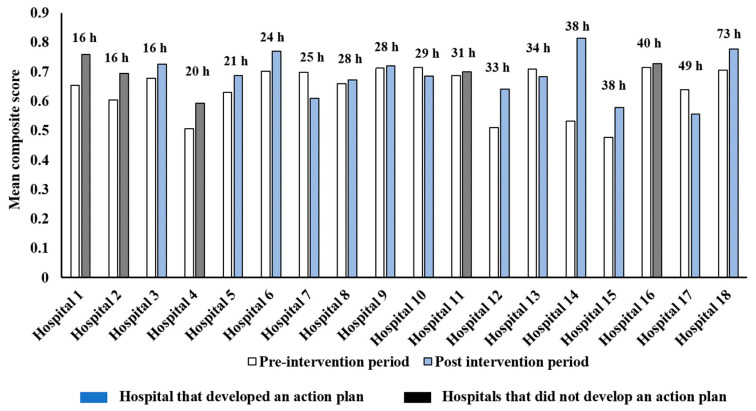
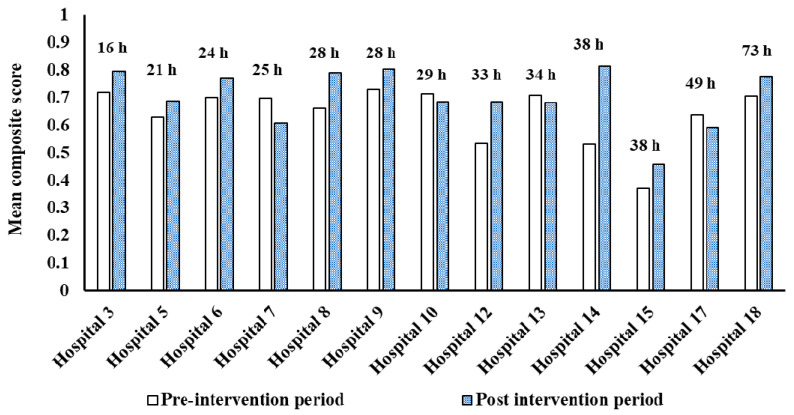
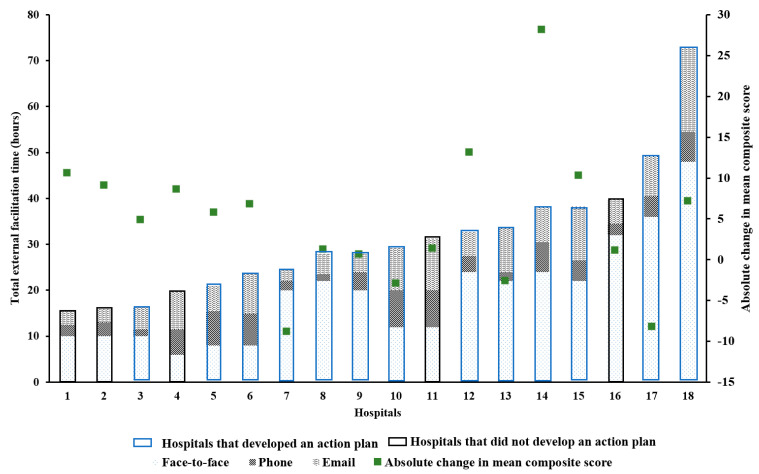
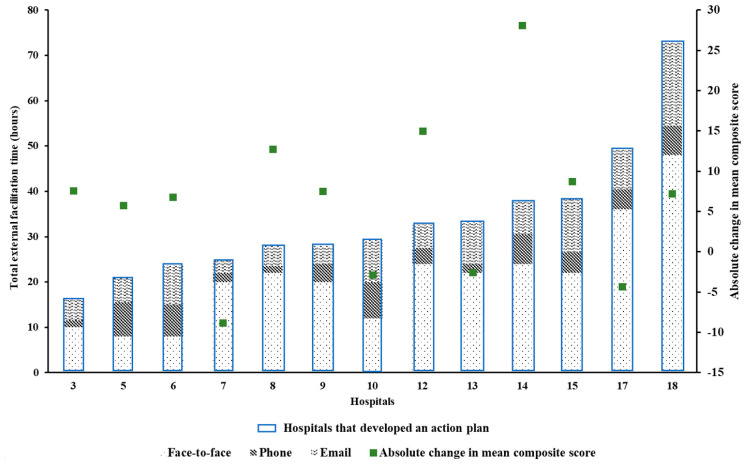
The use of external facilitation within the context of multicomponent quality improvement interventions (mQI) is growing. We aimed to evaluate the influence of external facilitation for improving the quality of acute stroke care. Clinicians from hospitals participating in mQI (Queensland, Australia) as part of the Stroke123 study were supported by external facilitators in a single, on-site workshop to review hospital performance against eight clinical processes of care (PoCs) collected in the Australian Stroke Clinical Registry (AuSCR) and develop an action plan. Remote support (i.e., telephone/email) after the workshop was provided. As part of a process evaluation for Stroke123, we recorded the number and mode of contacts between clinicians and facilitators; type of support provided; and frequency of self-directed, hospital-level stroke registry data reviews. Analysis: We measured the association between amount/type of external facilitation, (i) development of action plans, and (ii) adherence to PoCs before and after the intervention using AuSCR data from 2010 to 2015. In total, 14/19 hospitals developed an action plan. There was no significant difference in amount or type of external facilitator support provided between hospitals that did, and did not, develop an action plan. There was no relationship between the amount of external facilitation and change in adherence to PoCs. Most (95%) hospitals accessed stroke registry performance data. In the Stroke123 study, the amount or type of external facilitation did not influence action plan development, and the amount of support did not influence the changes achieved in adherence to PoCs. Remote support may not add value for mQI.
Keywords: behavior change intervention; facilitation; improvement science; process evaluation; quality improvement; stroke.
Conflict of interest statement
The authors declare the following potential conflicts of interest with respect to the research, authorship, and publication of this article: D.A.C. is the current Data Custodian for the Australian Stroke Clinical Registry (AuSCR). R.G. is the clinical lead for the Queensland State-wide Stroke Clinical Network and member Stroke Foundation Clinical Council. K.H. manages the Stroke Foundation’s National Stroke Audit and Stroke Clinical Guidelines programs. S.M., D.A.C., G.C., K.H. and R.G. are members of the AuSCR Steering or Management committees. S.M. was formerly a member of the NHMRC Research Committee but was appointed after this grant was awarded. The other authors report no conflicts.
Figures
References
-
- Brien E.C., Wu J., Zhao X., Schulte P.J., Fonarow G.C., Hernandez A.F., Schwamm L.H., Peterson E.D., Bhatt D.L., Smith E.E., et al. Healthcare Resource Availability, Quality of Care, and Acute Ischemic Stroke Outcomes. J. Am. Heart Assoc. 2017;6:e003813. doi: 10.1161/JAHA.116.003813. - DOI - PMC - PubMed
-
- Cadilhac D.A., Lannin N.A., Anderson C.S., Kim J., Andrew N., Kilkenny M., Shehata S., Grabsch B., Levi C., Faux S., et al. The Australian Stroke Clinical Registry Annual Report 2015. The Florey Institute of Neuroscience and Mental Health; 2016. Report No 7, pages 42.
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
