

Validity of Pneumonia Severity Assessment Scores in Africa and South Asia: A Systematic Review and Meta-Analysis
- PMID: 34574976
- PMCID: PMC8467534
- DOI: 10.3390/healthcare9091202
Validity of Pneumonia Severity Assessment Scores in Africa and South Asia: A Systematic Review and Meta-Analysis
Abstract
Background: Although community-acquired pneumonia (CAP) severity assessment scores are widely used, their validity in low- and middle-income countries (LMICs) is not well defined. We aimed to investigate the validity and performance of the existing scores among adults in LMICs (Africa and South Asia).
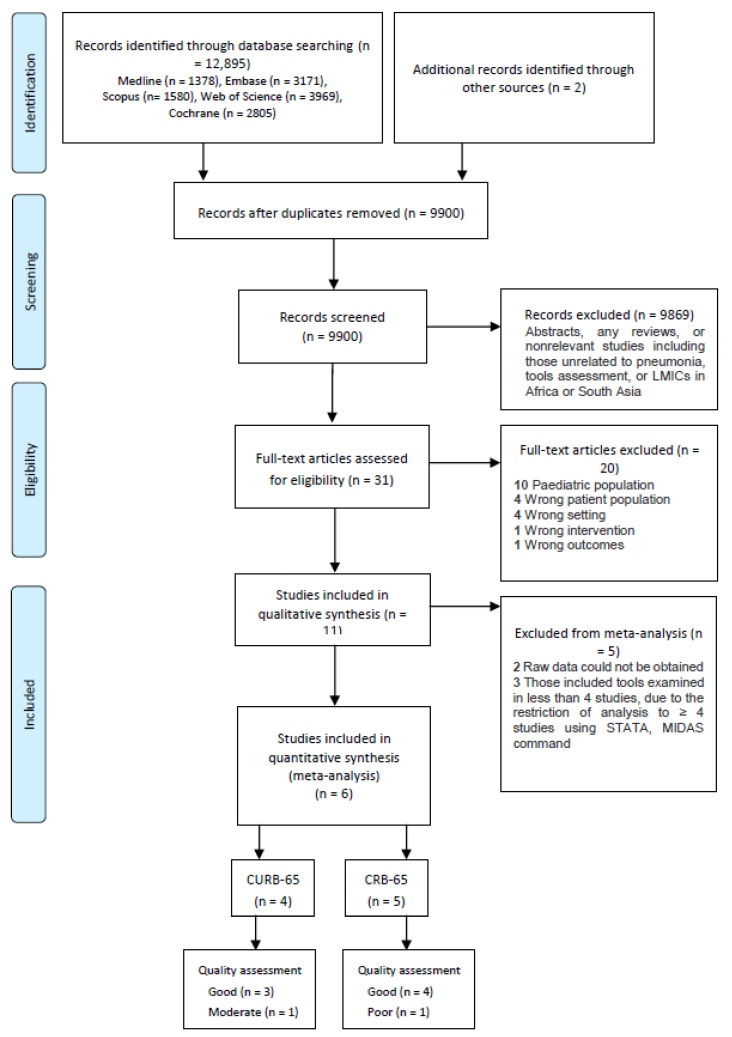
Methods: Medline, Embase, Cochrane Central Register of Controlled Trials, Scopus and Web of Science were searched to 21 May 2020. Studies evaluating a pneumonia severity score/tool among adults in these countries were included. A bivariate random-effects meta-analysis was performed to examine the scores' performance in predicting mortality.
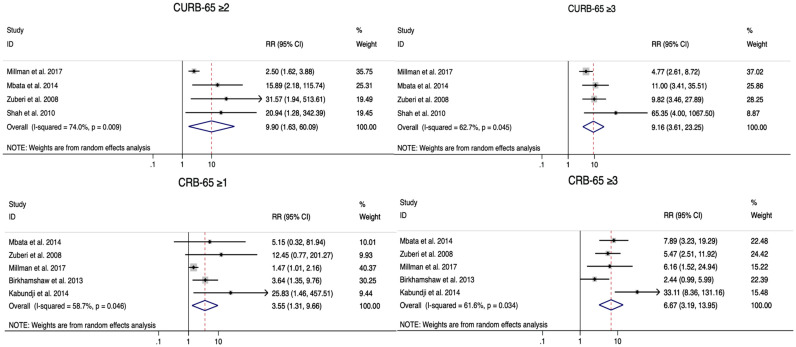
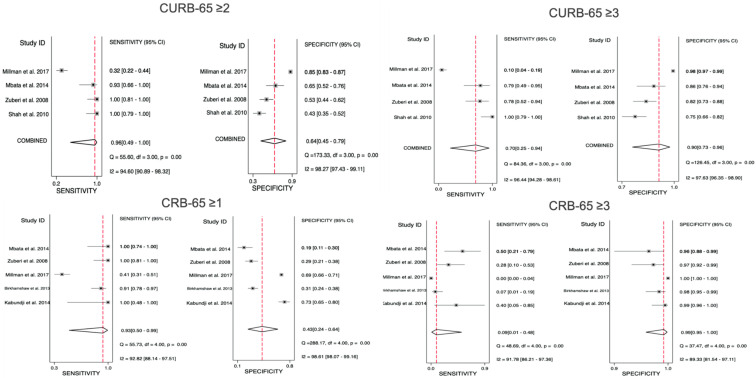
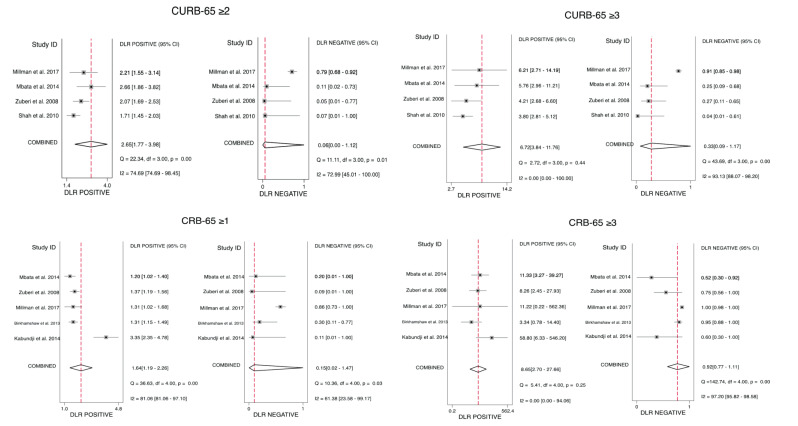
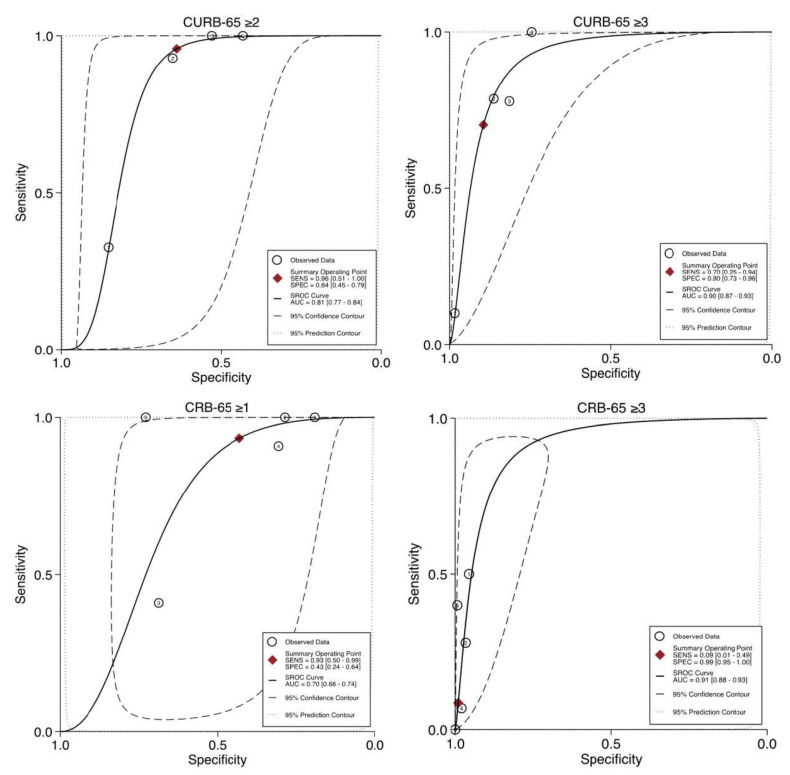
Results: Of 9900 records, 11 studies were eligible, covering 12 tools. Only CURB-65 (Confusion, Urea, Respiratory Rate, Blood Pressure, Age ≥ 65 years) and CRB-65 (Confusion, Respiratory Rate, Blood Pressure, Age ≥ 65 years) were included in the meta-analysis. Both scores were effective in predicting mortality risk. Performance characteristics (with 95% Confidence Interval (CI)) at high (CURB-65 ≥ 3, CRB-65 ≥ 3) and intermediate-risk (CURB-65 ≥ 2, CRB-65 ≥ 1) cut-offs were as follows: pooled sensitivity, for CURB-65, 0.70 (95% CI = 0.25-0.94) and 0.96 (95% CI = 0.49-1.00), and for CRB-65, 0.09 (95% CI = 0.01-0.48) and 0.93 (95% CI = 0.50-0.99); pooled specificity, for CURB-65, 0.90 (95% CI = 0.73-0.96) and 0.64 (95% CI = 0.45-0.79), and for CRB-65, 0.99 (95% CI = 0.95-1.00) and 0.43 (95% CI = 0.24-0.64).
Conclusions: CURB-65 and CRB-65 appear to be valid for predicting mortality in LMICs. CRB-65 may be employed where urea levels are unavailable. There is a lack of robust evidence regarding other scores, including the Pneumonia Severity Index (PSI).
Keywords: community-acquired pneumonia; developing countries; meta-analysis; mortality; prognosis; severity of illness index; systematic review.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Troeger C., Forouzanfar M., Rao P.C., Khalil I., Brown A., Swartz S., Fullman N., Mosser J., Thompson R.L., Reiner R.C., et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory tract infections in 195 countries: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect. Dis. 2017;17:1133–1161. doi: 10.1016/S1473-3099(17)30396-1. - DOI - PMC - PubMed
-
- Troeger C., Blacker B., Khalil I.A., Rao P.C., Cao J., Zimsen S.R.M., Albertson S.B., Deshpande A., Farag T., Abebe Z., et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018;18:1191–1210. doi: 10.1016/S1473-3099(18)30310-4. - DOI - PMC - PubMed
-
- Vos T., Allen C., Arora M., Barber R.M., Bhutta Z.A., Brown A., Carter A., Casey D.C., Charlson F.J., Chen A.Z., et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 Diseases and Injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–1858. - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
