

Metabolic Reprogramming and Host Tolerance: A Novel Concept to Understand Sepsis-Associated AKI
- PMID: 34575294
- PMCID: PMC8471000
- DOI: 10.3390/jcm10184184
Metabolic Reprogramming and Host Tolerance: A Novel Concept to Understand Sepsis-Associated AKI
Abstract
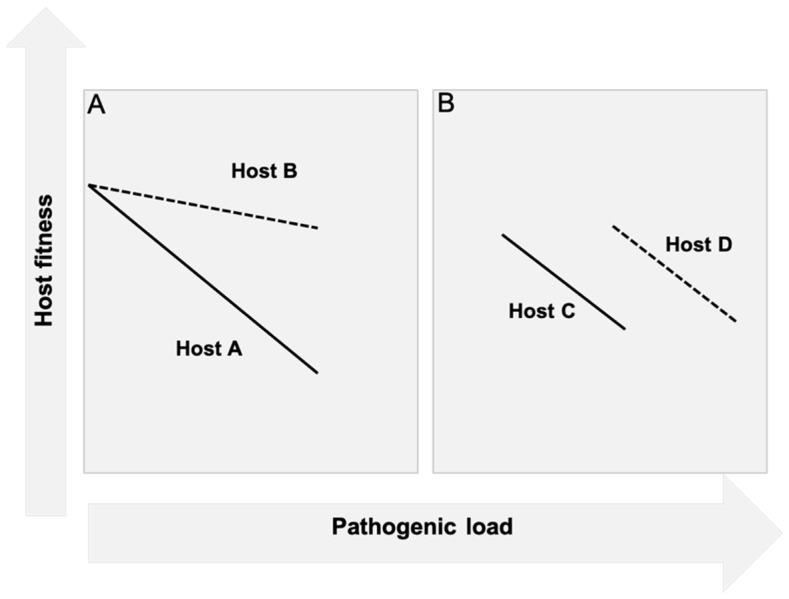
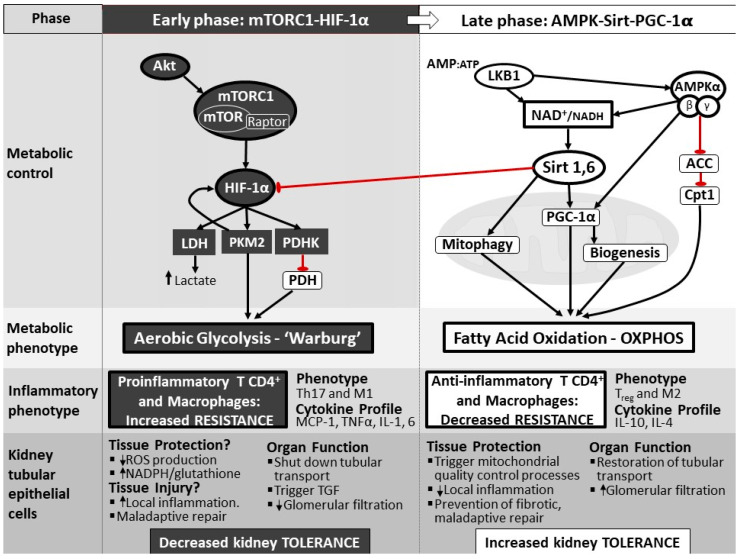
Acute kidney injury (AKI) is a frequent complication of sepsis that increases mortality and the risk of progression to chronic kidney disease. However, the mechanisms leading to sepsis-associated AKI are still poorly understood. The recognition that sepsis induces organ dysfunction in the absence of overt necrosis or apoptosis has led to the consideration that tubular epithelial cells (TEC) may deploy defense mechanisms to survive the insult. This concept dovetails well with the notion that the defense against infection does not only depend on the capacity of the immune system to limit the microbial load (known as resistance), but also on the capacity of cells and tissues to limit tissue injury (known as tolerance). In this review, we discuss the importance of TEC metabolic reprogramming as a defense strategy during sepsis, and how this cellular response is likely to operate through a tolerance mechanism. We discuss the fundamental role of specific regulatory nodes and of mitochondria in orchestrating this response, and how this opens avenues for the exploration of targeted therapeutic strategies to prevent or treat sepsis-associated AKI.
Keywords: AKI; metabolism; mitochondria; sepsis; tolerance.
Conflict of interest statement
The authors declare no conflict of interest in relation to this manuscript.
Figures
References
-
- Singer M., Deutschman C.S., Seymour C.W., Shankar-Hari M., Annane D., Bauer M., Bellomo R., Bernard G.R., Chiche J.D., Coopersmith C.M., et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) JAMA. 2016;315:801–810. doi: 10.1001/jama.2016.0287. - DOI - PMC - PubMed
-
- Rudd K.E., Johnson S.C., Agesa K.M., Shackelford K.A., Tsoi D., Kievlan D.R., Colombara D.V., Ikuta K.S., Kissoon N., Finfer S., et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: Analysis for the Global Burden of Disease Study. Lancet. 2020;395:200–211. doi: 10.1016/S0140-6736(19)32989-7. - DOI - PMC - PubMed
-
- Kellum J.A., Chawla L.S., Keener C., Singbartl K., Palevsky P.M., Pike F.L., Yealy D.M., Huang D.T., Angus D.C., ProCESS and ProGReSS-AKI Investigators The Effects of Alternative Resuscitation Strategies on Acute Kidney Injury in Patients with Septic Shock. Am. J. Respir. Crit. Care Med. 2016;193:281–287. doi: 10.1164/rccm.201505-0995OC. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
