

Application of a 72 h National Early Warning Score and Incorporation with Sequential Organ Failure Assessment for Predicting Sepsis Outcomes and Risk Stratification in an Intensive Care Unit: A Derivation and Validation Cohort Study
- PMID: 34575690
- PMCID: PMC8465191
- DOI: 10.3390/jpm11090910
Application of a 72 h National Early Warning Score and Incorporation with Sequential Organ Failure Assessment for Predicting Sepsis Outcomes and Risk Stratification in an Intensive Care Unit: A Derivation and Validation Cohort Study
Abstract
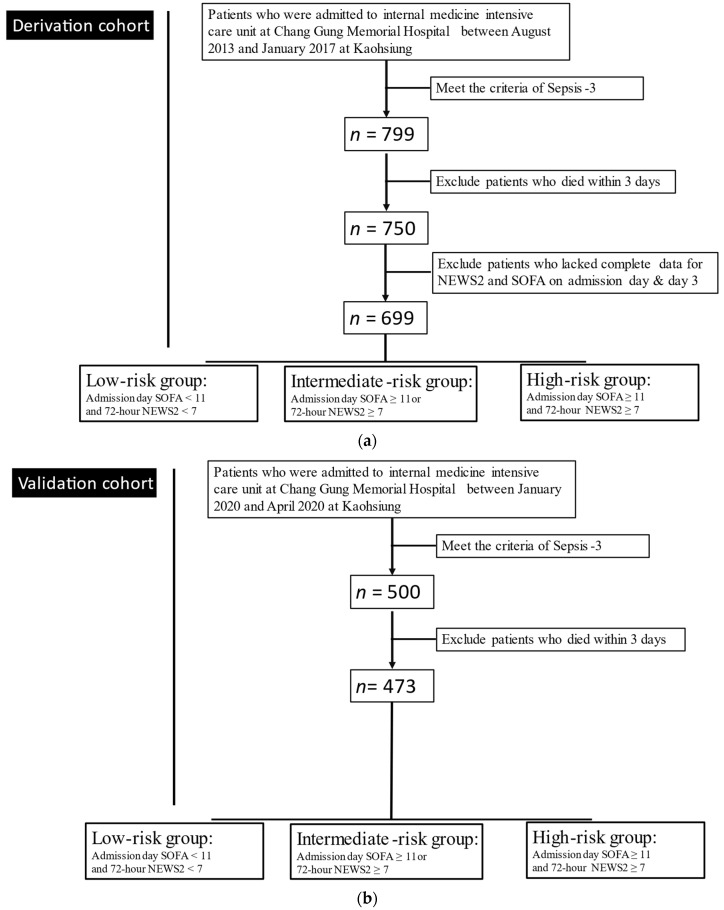
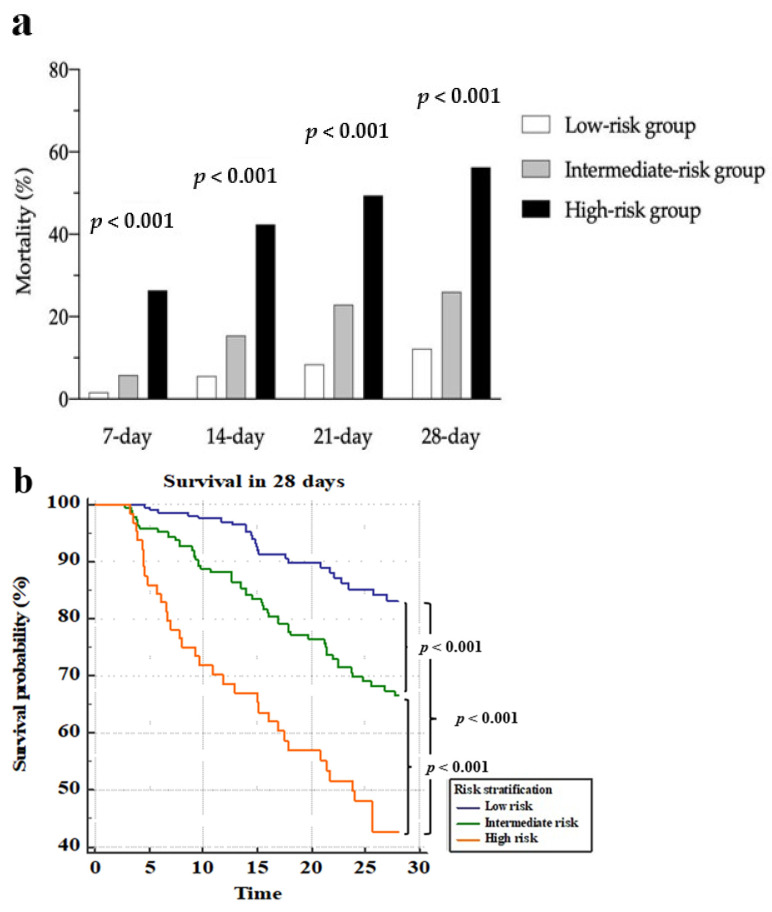
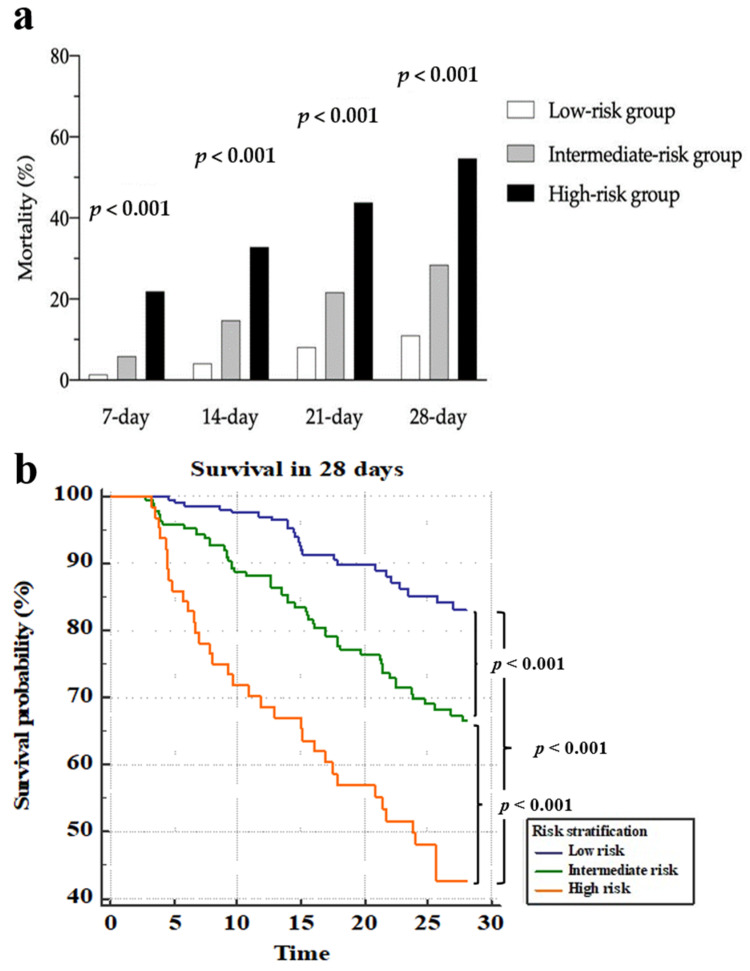
We investigated the best timing for using the National Early Warning Score 2 (NEWS2) for predicting sepsis outcomes and whether combining the NEWS2 and the Sequential Organ Failure Assessment (SOFA) was applicable for mortality risk stratification in intensive care unit (ICU) patients with severe sepsis. All adult patients who met the Third International Consensus Definitions for Sepsis and Septic Shock criteria between August 2013 and January 2017 with complete clinical parameters and laboratory data were enrolled as a derivation cohort. The primary outcomes were the 7-, 14-, 21-, and 28-day mortalities. Furthermore, another group of patients under the same setting between January 2020 and March 2020 were also enrolled as a validation cohort. In the derivation cohort, we included 699 consecutive adult patients. The 72 h NEWS2 had good discrimination for predicting 7-, 14-, 21-, and 28-day mortalities (AUC: 0.780, 0.724, 0.700, and 0.667, respectively) and was not inferior to the SOFA (AUC: 0.740, 0.680, 0.684, and 0.677, respectively). With the new combined NESO tool, the hazard ratio was 1.854 (1.203-2.950) for the intermediate-risk group and 6.810 (3.927-11.811) for the high-risk group relative to the low-risk group. This finding was confirmed in the validation cohort using a separated survival curve for 28-day mortality. The 72 h NEWS2 alone was non-inferior to the admission SOFA or day 3 SOFA for predicting sepsis outcomes. The NESO tool was found to be useful for 7-, 14-, 21-, and 28-day mortality risk stratification in patients with severe sepsis.
Keywords: National Early Warning Score 2; Sequential Organ Failure Assessment; intensive care unit; mortality risk stratification; severe sepsis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Murphy S.L., Kochanek K.D., Xu J. Deaths: Final data for 2011. Natl. Vital Stat. Rep. 2015;63:3. - PubMed
-
- Sakr Y., Jaschinski U., Wittebole X., Szakmany T., Lipman J., Ñamendys-Silva S.A., Martin-Loeches I., Leone M., Lupu M.-N., Vincent J.-L. Sepsis in intensive care unit patients: Worldwide data from the intensive care over nations audit. Open Forum Infect. Dis. 2018;5:ofy313. doi: 10.1093/ofid/ofy313. - DOI - PMC - PubMed
-
- Seymour C.W., Liu V.X., Iwashyna T.J., Brunkhorst F.M., Rea T.D., Scherag A., Rubenfeld G., Kahn J.M., Shankar-Hari M., Singer M.J.J. Assessment of clinical criteria for sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) Jama. 2016;315:762–774. doi: 10.1001/jama.2016.0288. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
