

Evaluating Change of Marginal Bone Height with Cone-Beam Computed Tomography Following Surgical Treatment with Guided Tissue Regeneration (Bone Grafting) or Access Flap Alone: A Retrospective Study
- PMID: 34577792
- PMCID: PMC8472387
- DOI: 10.3390/medicina57090869
Evaluating Change of Marginal Bone Height with Cone-Beam Computed Tomography Following Surgical Treatment with Guided Tissue Regeneration (Bone Grafting) or Access Flap Alone: A Retrospective Study
Abstract
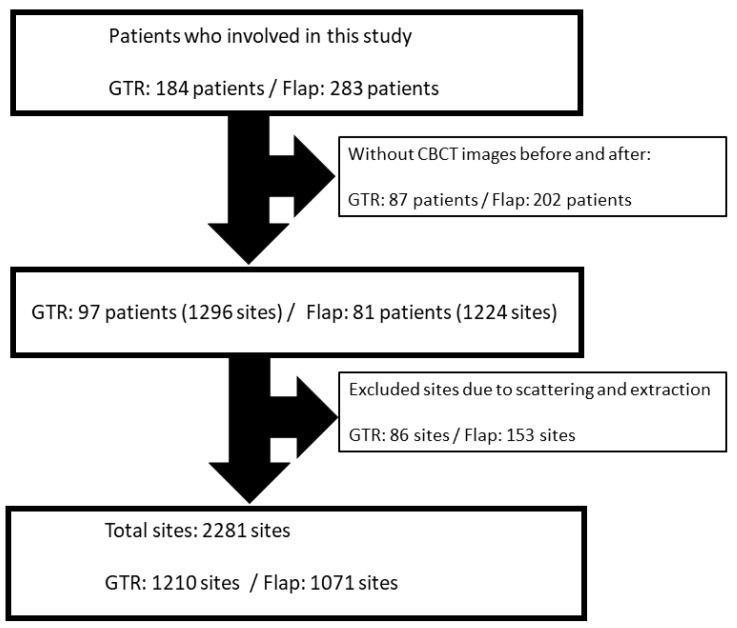
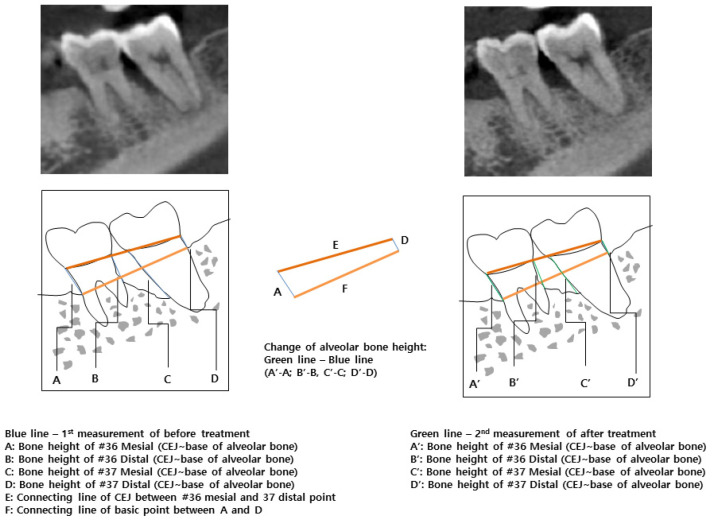
Background and Objectives: This study aimed to evaluate the change of bone height following treatment of human intrabony defects with guided tissue regeneration (GTR) with bone grafting or access flap alone by cone-beam computed tomography (CBCT) scan. Materials and methods: This study was conducted as a retrospective longitudinal study. In this study, a total of 2281 teeth sites were included: the GTR group had 1210 sites, and the Flap group had 1071 sites. In the GTR group, demineralized freeze-dried bone (DFDBA) particles in combination with resorbable collagen membrane were used. No regenerative material was applied to the Flap group. CBCT images were taken twice at baseline and at least 2.5 months postoperatively. Bone heights were measured using software on CBCT images. Results: The bony change between the GTR and Flap groups was significantly different (p = 0.00001). Both males and females in the GTR group had smaller bone loss than in the Flap group. In age groups, significant differences of bony height between the GTR and Flap groups were observed in the subgroups consisting of those 29-45 and 46-53 years old. The non-smoking subjects in the GTR group had higher bone heights than those in the Flap group. In the absence of systemic disease and medicine, bone formation was higher in the GTR group than in the Flap group. In terms of oral position, the #14-17, #34-37, and #44-47 subgroups of the GTR group showed higher levels of bone heights than those of the Flap group. Conclusions. The results of this study indicated that the GTR procedure offers the additional benefit of higher bone heights than the Flap procedure does.
Keywords: dental materials; guided tissue regeneration; osseous defects; periodontal regeneration; periodontal surgery; periodontitis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Comparison of 2 regenerative procedures--guided tissue regeneration and demineralized freeze-dried bone allograft--in the treatment of intrabony defects: a clinical and radiographic study.J Periodontol. 1998 Jul;69(7):751-8. doi: 10.1902/jop.1998.69.7.751. J Periodontol. 1998. PMID: 9706851
-
Five-year clinical results for treatment of intrabony defects with EMD, guided tissue regeneration and open-flap debridement: a case series.J Periodontal Res. 2015 Feb;50(1):123-30. doi: 10.1111/jre.12188. Epub 2014 May 12. J Periodontal Res. 2015. PMID: 24815103
-
Treatment of intraosseous defects with bioabsorbable barriers alone or in combination with decalcified freeze-dried bone allograft: a randomized clinical trial.J Periodontol. 2000 Dec;71(12):1852-61. doi: 10.1902/jop.2000.71.12.1852. J Periodontol. 2000. PMID: 11156042 Clinical Trial.
-
Histologic evidence of periodontal regeneration in furcation defects: a systematic review.Clin Oral Investig. 2019 Jul;23(7):2861-2906. doi: 10.1007/s00784-019-02964-3. Epub 2019 Jun 4. Clin Oral Investig. 2019. PMID: 31165313
-
Predictability of clinical outcomes following regenerative therapy in intrabony defects.J Periodontol. 2008 Mar;79(3):387-93. doi: 10.1902/jop.2008.060521. J Periodontol. 2008. PMID: 18315419 Review.
Cited by
-
Assessment of Bone Height Changes Based on the Cone-Beam Computed Tomography Following Intentional Replantation for Periodontally Compromised Teeth.Medicina (Kaunas). 2022 Dec 25;59(1):40. doi: 10.3390/medicina59010040. Medicina (Kaunas). 2022. PMID: 36676664 Free PMC article.
-
Eggshell Derived Nanohydroxyapatite as a Bone Graft for Intrabony Defects was Evaluated Using (CBCT) - A Randomized Controlled Trial.J Pharm Bioallied Sci. 2024 Dec;16(Suppl 5):S4517-S4521. doi: 10.4103/jpbs.jpbs_1041_24. Epub 2025 Jan 30. J Pharm Bioallied Sci. 2024. PMID: 40061730 Free PMC article.
-
Regeneration of Intrabony Defects Using a Novel Magnesium Membrane.Medicina (Kaunas). 2023 Nov 16;59(11):2018. doi: 10.3390/medicina59112018. Medicina (Kaunas). 2023. PMID: 38004067 Free PMC article.
-
Beyond Bone Grafts: Exploring the Efficacy of Alternative Regenerative Therapies.Cureus. 2024 Nov 15;16(11):e73745. doi: 10.7759/cureus.73745. eCollection 2024 Nov. Cureus. 2024. PMID: 39677141 Free PMC article.
-
Biomaterials for Periodontal Regeneration.Dent Clin North Am. 2022 Oct;66(4):659-672. doi: 10.1016/j.cden.2022.05.011. Epub 2022 Sep 11. Dent Clin North Am. 2022. PMID: 36216452 Free PMC article. Review.
References
-
- Lang N.P., Lindhe J. Clinical Periodontology and Implant Dentistry. 5th ed. John Wiley & Sons; New York, NY, USA: 2015. pp. 783–786.
-
- Nevins M.L., Camelo M., Lynch S.E., Schenk R.K., Nevins M. Evaluation of periodontal regeneration following grafting intrabony defects with bio-oss collagen: A human histologic report. Int. J. Periodontics Restor. Dent. 2003;23:9–17. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
