

Acrometastases to the Hand: A Systematic Review
- PMID: 34577873
- PMCID: PMC8471162
- DOI: 10.3390/medicina57090950
Acrometastases to the Hand: A Systematic Review
Abstract
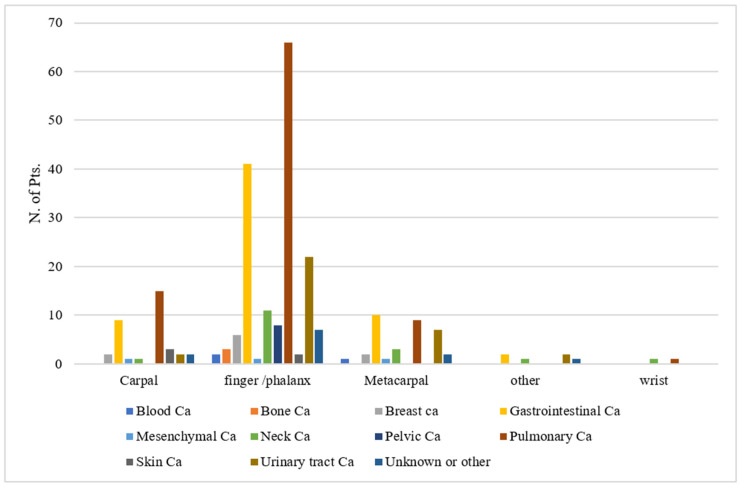
Background and Objectives: The term acrometastases (AM) refers to secondary lesions sited distally to the elbow and knee, representing 0.1% of all bony metastases. By frequency, pulmonary cancer and gastrointestinal and genitourinary tract neoplasms are the most responsible for the reported AM. Improvements in oncologic patient care favor an increase in the incidence of such rare cases. We performed a systematic review of acrometastases to the hand to provide further insight into the management of these fragile patients. We also present a peculiar case of simultaneous acrometastasis to the ring finger and pathological vertebral fracture. Material and Methods: A literature search according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement was conducted using the PubMed, Google Scholar, and Scopus databases in December 2020 on metastasis to the hand and wrist, from 1986 to 2020. MeSH terms included acrometastasis, carpal metastasis, hand metastasis, finger metastasis, phalangeal metastasis, and wrist metastasis. Results: In total, 215 studies reporting the follow-up of 247 patients were analyzed, with a median age of 62 years (range 10-91 years). Overall, 162 out of 247 patients were males (65.6%) and 85 were females (34.4%). The median reported follow-up was 5 months (range 0.5-39). The median time from primary tumor diagnosis to acrometastasis was 24 months (range 0.7-156). Acrometastases were located at the finger/phalanx (68.4%), carpal (14.2%), metacarpal (14.2%), or other sites (3.2%). The primary tumors were pulmonary in 91 patients (36.8%). The average interval from primary tumor diagnosis to acrometastasis varied according to the primary tumor type from 2 months (in patients with mesenchymal tumors) to 64.0 months (in patients with breast cancer). Conclusions: Acrometastases usually develop in the late stage of oncologic disease and are associated with short life expectancy. Their occurrence can no longer be considered rare; physicians should thus be updated on their surgical management and their impact on prognosis and survival.
Keywords: acrometastases; carcinoma; chemotherapy; immunotherapy; radiotherapy; thumb metastases.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Stomeo D., Tulli A., Ziranu A., Perisano C., De Santis V., Maccauro G. Acrometastasis: A literature review. Eur. Rev. Med. Pharmacol. Sci. 2015;19:2906–2915. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
