

The Clamshell Osteotomy for Diaphyseal Malunion in Deformity Correction and Fracture Surgery
- PMID: 34577874
- PMCID: PMC8468248
- DOI: 10.3390/medicina57090951
The Clamshell Osteotomy for Diaphyseal Malunion in Deformity Correction and Fracture Surgery
Abstract
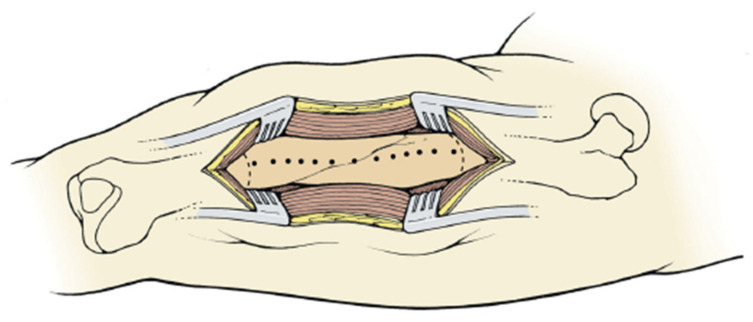
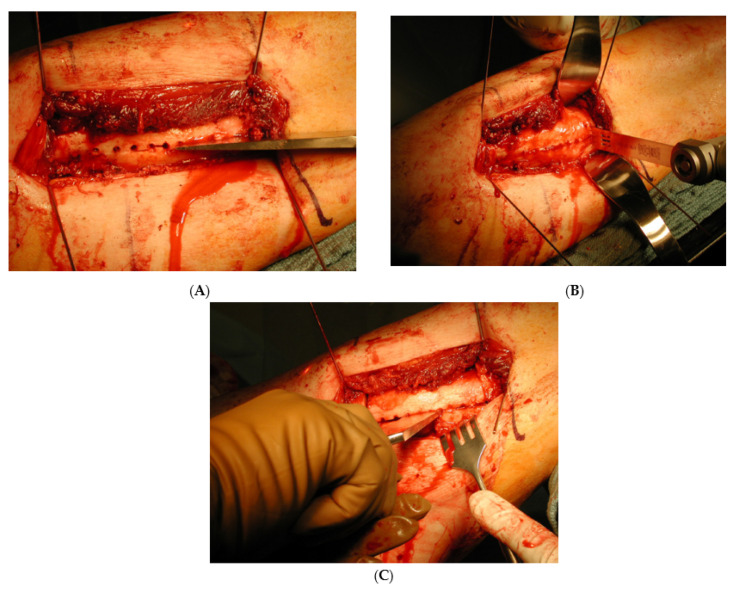
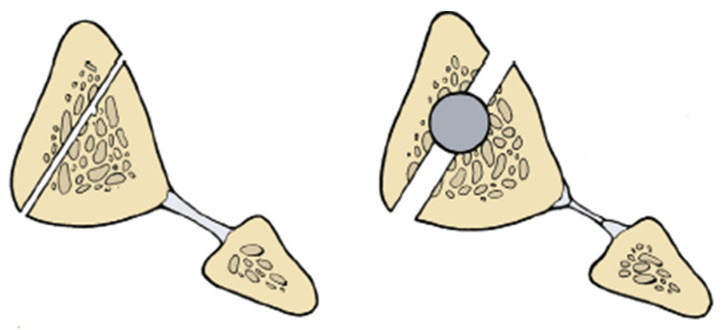
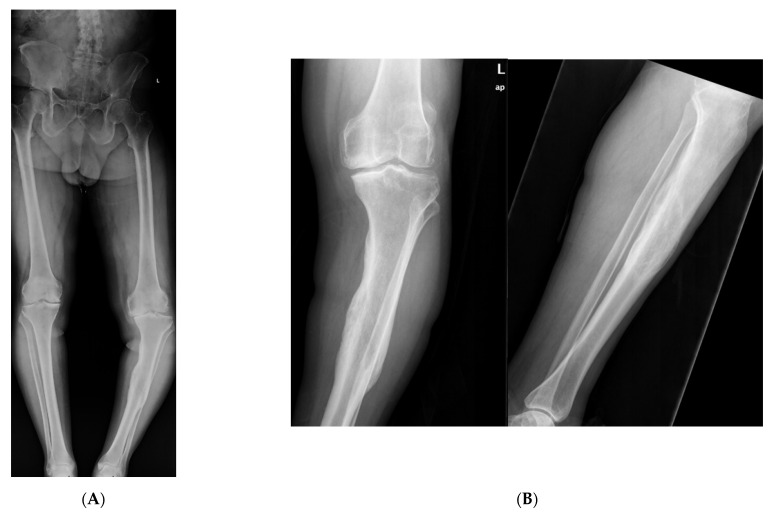
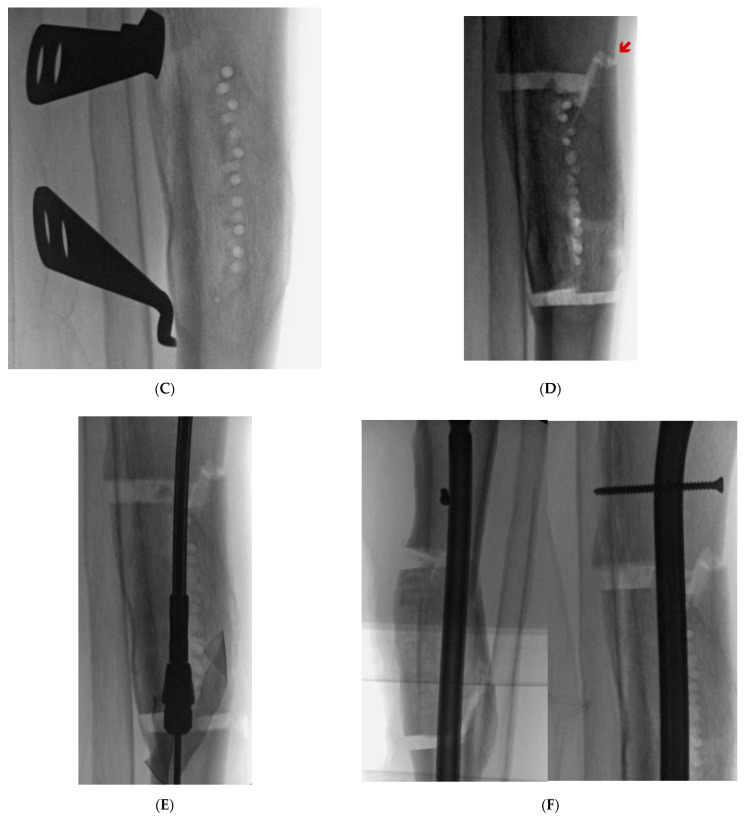
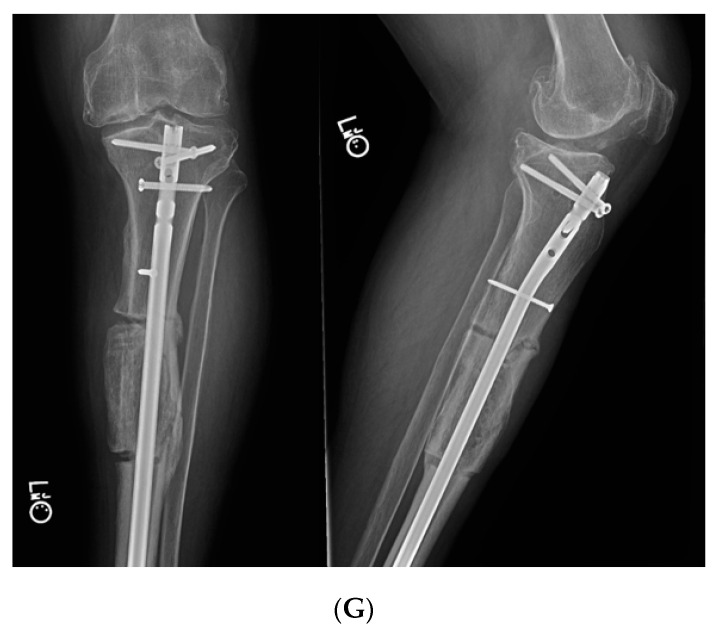
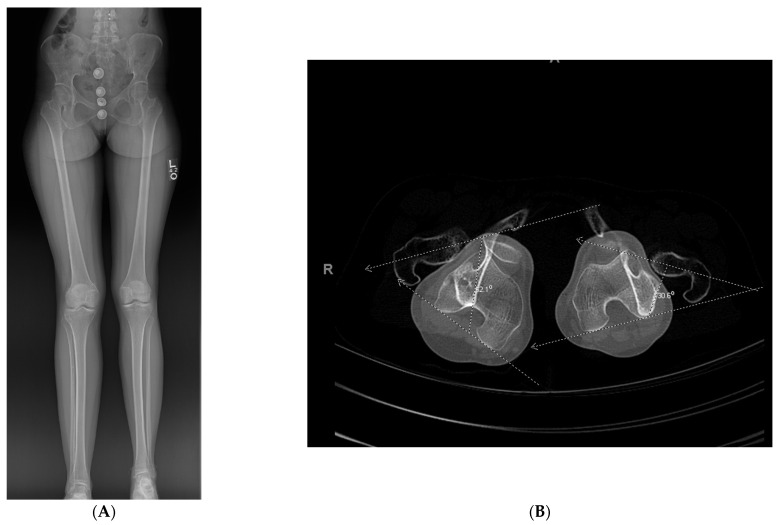
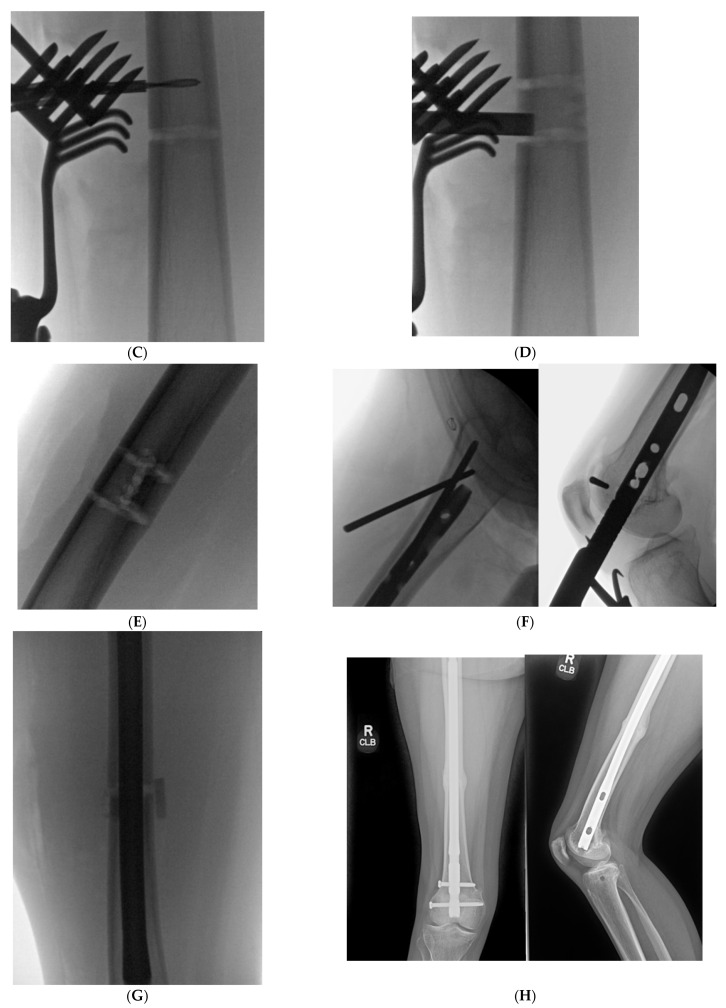
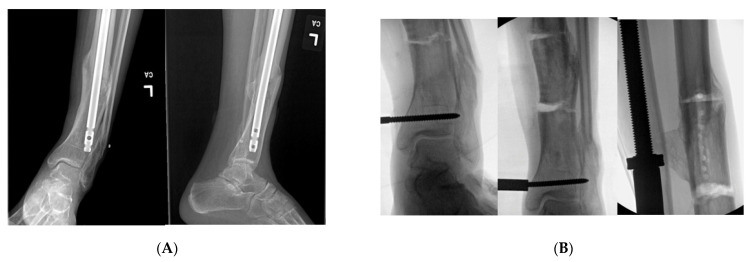
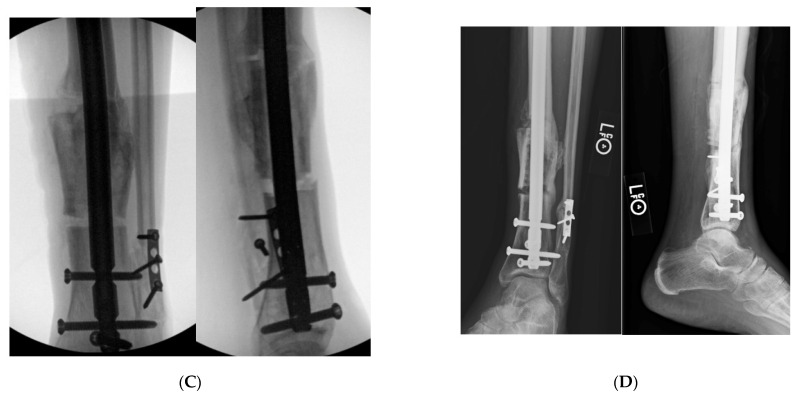
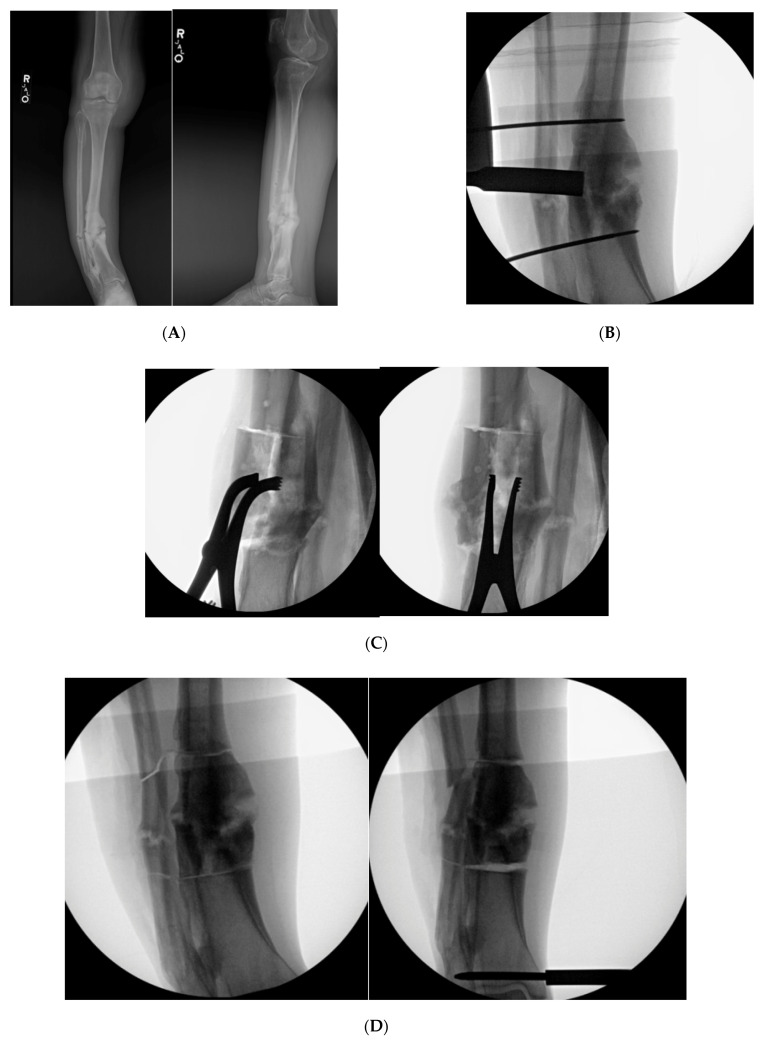
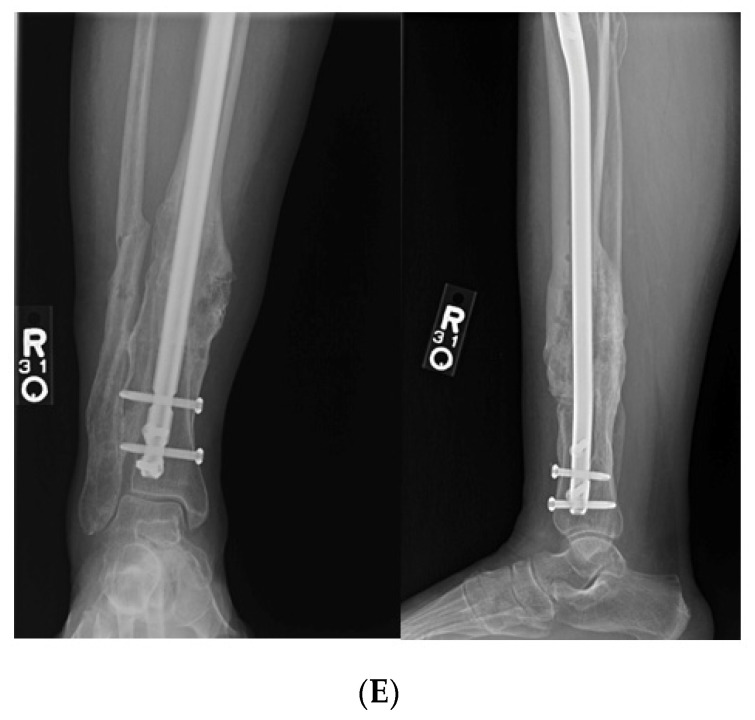
Diaphyseal malunion poses a great challenge for the orthopedic surgeon, and an inundation of morbidity for the patient. Diaphyseal malunion can cause altered gait, adjacent joint osteoarthritis and body dissatisfaction. This problem is fraught with complications without surgical intervention. There is a myriad of options for the management of a diaphyseal malunion. The clamshell osteotomy was engendered to ameliorate the difficulty in managing this issue. This technique is a viable option to correct diaphyseal malunion about the femur and tibia. Recently, the indications of a clamshell osteotomy have been expanded to function as a derotational or shortening osteotomy.
Keywords: clamshell; deformity; diaphyseal; femur; fracture; malunion; nonunion; osteotomy; tibia.
Conflict of interest statement
All authors declare no conflict of interest with regards to this publication.
Figures
References
-
- Giannoudis P.V., Christoph Pape H., Schütz M. Antegrade Nailing Approach with Piriformis Entry Point. [(accessed on 29 June 2021)]. Available online: https://surgeryreference.aofoundation.org/orthopedic-trauma/adult-trauma....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
