

The Gut Microbiota during a Behavioral Weight Loss Intervention
- PMID: 34579125
- PMCID: PMC8471894
- DOI: 10.3390/nu13093248
The Gut Microbiota during a Behavioral Weight Loss Intervention
Abstract
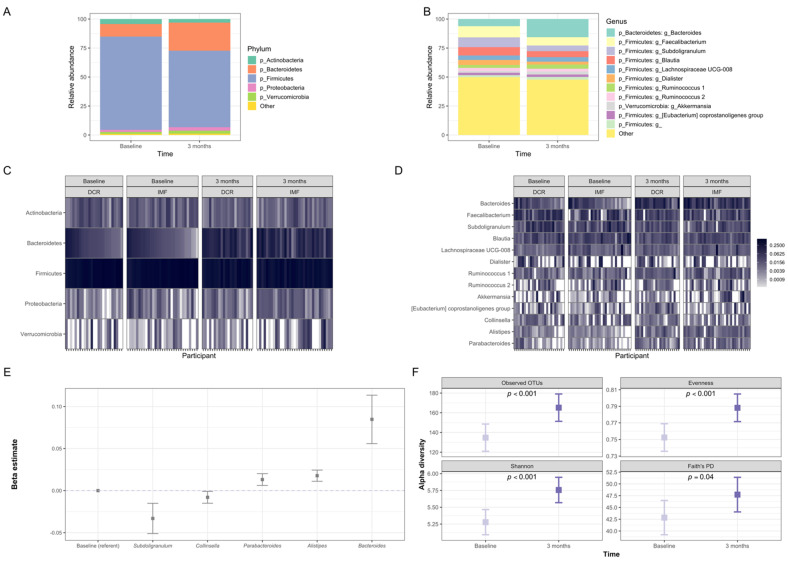
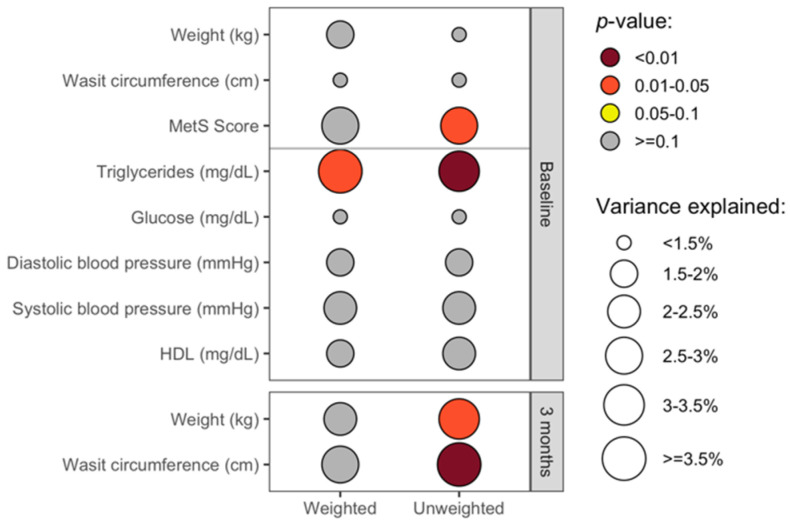
Altered gut microbiota has been linked to obesity and may influence weight loss. We are conducting an ongoing weight loss trial, comparing daily caloric restriction (DCR) to intermittent fasting (IMF) in adults who are overweight or obese. We report here an ancillary study of the gut microbiota and selected obesity-related parameters at the baseline and after the first three months of interventions. During this time, participants experienced significant improvements in clinical health measures, along with altered composition and diversity of fecal microbiota. We observed significant associations between the gut microbiota features and clinical measures, including weight and waist circumference, as well as changes in these clinical measures over time. Analysis by intervention group found between-group differences in the relative abundance of Akkermansia in response to the interventions. Our results provide insight into the impact of baseline gut microbiota on weight loss responsiveness as well as the early effects of DCR and IMF on gut microbiota.
Keywords: intermittent fasting; microbiota; obesity; weight loss.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- Virani Salim S., Alvaro A., Benjamin Emelia J., Bittencourt Marcio S., Callaway Clifton W., Carson April P., Chamberlain Alanna M., Chang Alexander R., Cheng S., Delling Francesca N., et al. Heart Disease and Stroke Statistics—2020 Update: A Report From the American Heart Association. Circulation. 2020;141:e139–e596. doi: 10.1161/CIR.0000000000000757. - DOI - PubMed
-
- Jensen M.D., Ryan D.H., Apovian C.M., Ard J.D., Comuzzie A.G., Donato K.A., Hu F.B., Hubbard V.S., Jakicic J.M., Kushner R.F., et al. 2013 AHA/ACC/TOS Guideline for the Management of Overweight and Obesity in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. J. Am. Coll. Cardiol. 2014;63:2985–3023. doi: 10.1016/j.jacc.2013.11.004. - DOI - PubMed
