

Prognostic Value of Electrocardiographic QRS Diminution in Patients Hospitalized With COVID-19 or Influenza
- PMID: 34579830
- PMCID: PMC8349698
- DOI: 10.1016/j.amjcard.2021.07.048
Prognostic Value of Electrocardiographic QRS Diminution in Patients Hospitalized With COVID-19 or Influenza
Abstract
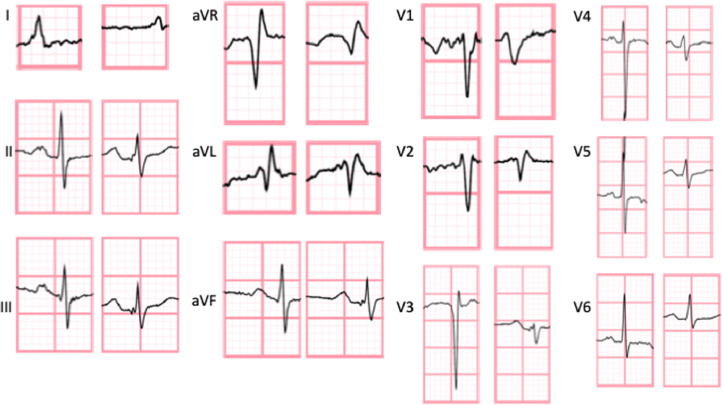
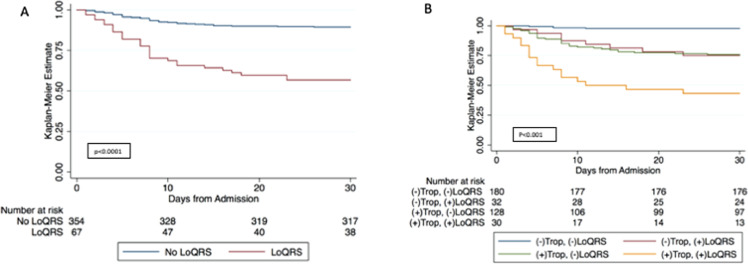
During the clinical care of hospitalized patients with COVID-19, diminished QRS amplitude on the surface electrocardiogram (ECG) was observed to precede clinical decompensation, culminating in death. This prompted investigation into the prognostic utility and specificity of low QRS complex amplitude (LoQRS) in COVID-19. We retrospectively analyzed consecutive adults admitted to a telemetry service with SARS-CoV-2 (n = 140) or influenza (n = 281) infection with a final disposition-death or discharge. LoQRS was defined as a composite of QRS amplitude <5 mm or <10 mm in the limb or precordial leads, respectively, or a ≥50% decrease in QRS amplitude on follow-up ECG during hospitalization. LoQRS was more prevalent in patients with COVID-19 than influenza (24.3% vs 11.7%, p = 0.001), and in patients who died than survived with either COVID-19 (48.1% vs 10.2%, p <0.001) or influenza (38.9% vs 9.9%, p <0.001). LoQRS was independently associated with mortality in patients with COVID-19 when adjusted for baseline clinical variables (odds ratio [OR] 11.5, 95% confidence interval [CI] 3.9 to 33.8, p <0.001), presenting and peak troponin, D-dimer, C-reactive protein, albumin, intubation, and vasopressor requirement (OR 13.8, 95% CI 1.3 to 145.5, p = 0.029). The median time to death in COVID-19 from the first ECG with LoQRS was 52 hours (interquartile range 18 to 130). Dynamic QRS amplitude diminution is a strong independent predictor of death over not only the course of COVID-19 infection, but also influenza infection. In conclusion, this finding may serve as a pragmatic prognostication tool reflecting evolving clinical changes during hospitalization, over a potentially actionable time interval for clinical reassessment.
Copyright © 2021 Elsevier Inc. All rights reserved.
Figures
References
-
- Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, Xiang J, Wang Y, Song B, Gu X, Guan L, Wei Y, Li H, Wu X, Xu J, Tu S, Zhang Y, Chen H, Cao B. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395:1054–1062. - PMC - PubMed
-
- Lala A, Johnson KW, Januzzi JL, Russak AJ, Paranjpe I, Richter F, Zhao S, Somani S, Van Vleck T, Vaid A, Chaudhry F, De Freitas JK, Fayad ZA, Pinney SP, Levin M, Charney A, Bagiella E, Narula J, Glicksberg BS, Nadkarni G, Mancini DM, Fuster V. Prevalence and impact of myocardial injury in patients hospitalized with COVID-19 infection. J Am Coll Cardiol. 2020;76:533–546. - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
