

Organoids Derived from Neoadjuvant FOLFIRINOX Patients Recapitulate Therapy Resistance in Pancreatic Ductal Adenocarcinoma
- PMID: 34580113
- PMCID: PMC9401459
- DOI: 10.1158/1078-0432.CCR-21-1681
Organoids Derived from Neoadjuvant FOLFIRINOX Patients Recapitulate Therapy Resistance in Pancreatic Ductal Adenocarcinoma
Abstract
Purpose: We investigated whether organoids can be generated from resected tumors of patients who received eight cycles of neoadjuvant FOLFIRINOX chemotherapy before surgery, and evaluated the sensitivity/resistance of these surviving cancer cells to cancer therapy.
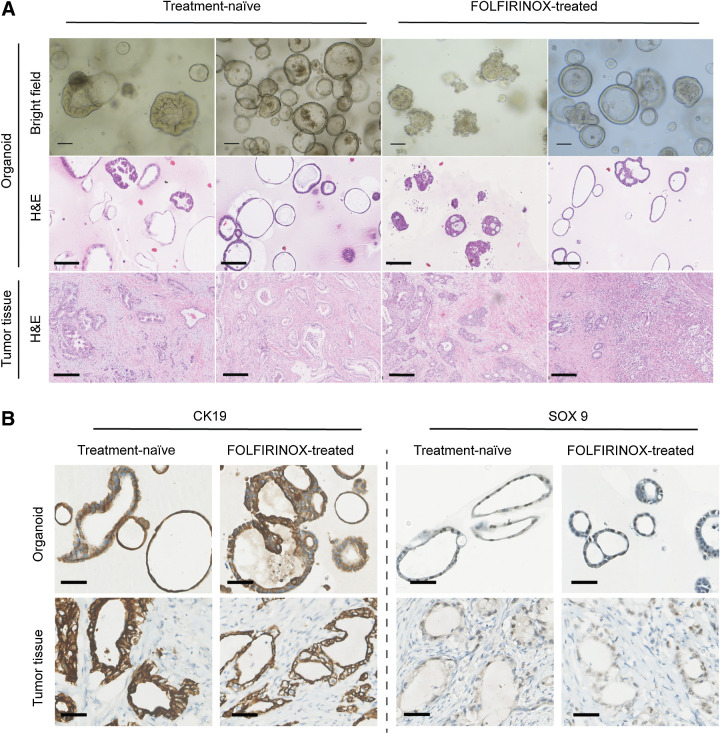
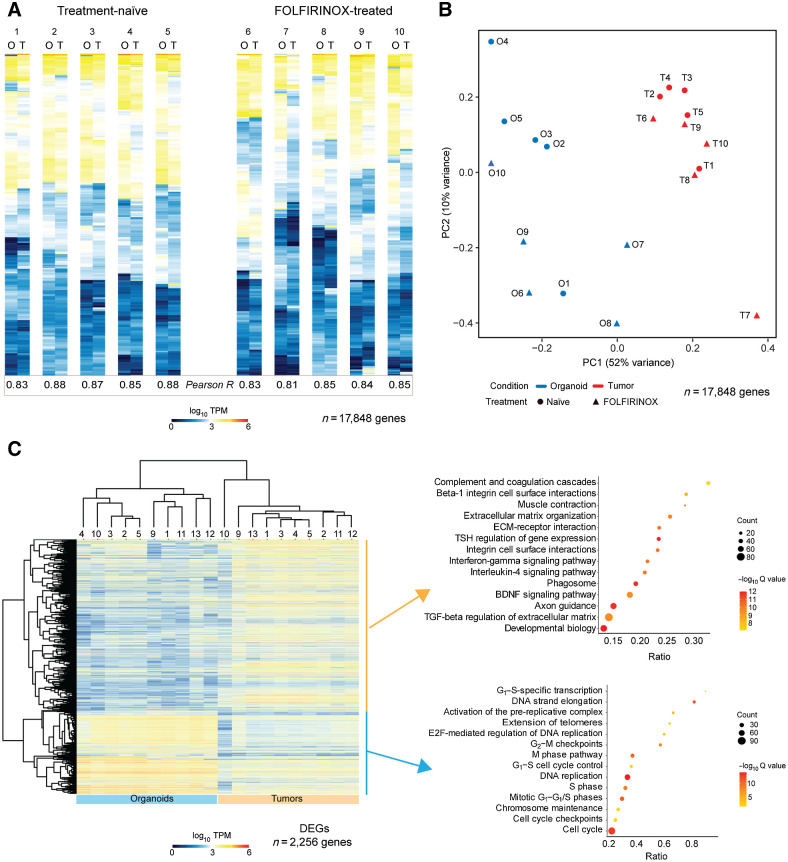
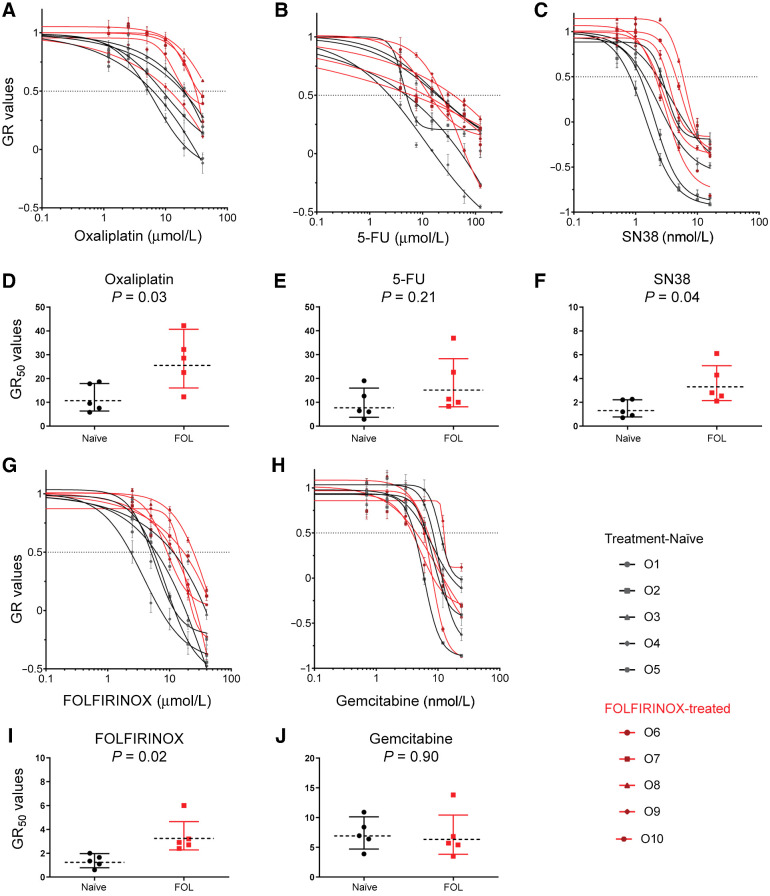
Experimental design: We generated a library of 10 pancreatic ductal adenocarcinoma (PDAC) organoid lines: five each from treatment-naïve and FOLFIRINOX-treated patients. We first assessed the histologic, genetic, and transcriptional characteristics of the organoids and their matched primary PDAC tissue. Next, the organoids' response to treatment with single agents-5-FU, irinotecan, and oxaliplatin-of the FOLFIRINOX regimen as well as combined regimen was evaluated. Finally, global mRNA-seq analyses were performed to identify FOLFIRINOX resistance pathways.
Results: All 10 patient-derived PDAC organoids recapitulate histologic, genetic, and transcriptional characteristics of their primary tumor tissue. Neoadjuvant FOLFIRINOX-treated organoids display resistance to FOLFIRINOX (5/5), irinotecan (5/5), and oxaliplatin (4/5) when compared with treatment-naïve organoids (FOLFIRINOX: 1/5, irinotecan: 2/5, oxaliplatin: 0/5). 5-Fluorouracil treatment responses between naïve and treated organoids were similar. Comparative global transcriptome analysis of treatment-naïve and FOLFIRINOX samples-in both organoids and corresponding matched tumor tissues-uncovered modulated pathways mainly involved in genomic instability, energy metabolism, and innate immune system.
Conclusions: Resistance development in neoadjuvant FOLFIRINOX organoids, recapitulating their primary tumor resistance, suggests continuation of FOLFIRINOX therapy as an adjuvant treatment may not be advantageous for these patients. Gene-expression profiles of PDAC organoids identify targetable pathways involved in chemoresistance development upon neoadjuvant FOLFIRINOX treatment, thus opening up combination therapy possibilities.
©2021 The Authors; Published by the American Association for Cancer Research.
Figures


References
-
- Oettle H, Neuhaus P, Hochhaus A, Hartmann JT, Gellert K, Ridwelski K, et al. Adjuvant chemotherapy with gemcitabine and long-term outcomes among patients with resected pancreatic cancer: the CONKO-001 randomized trial. JAMA 2013;310:1473. - PubMed
-
- Khorana AA, Mangu PB, Berlin J, Engebretson A, Hong TS, Maitra A, et al. Potentially curable pancreatic cancer: American Society of Clinical Oncology Clinical Practice Guideline. JCO 2016;34:2541–56. - PubMed
-
- Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 2011;364:1817–25. - PubMed
-
- Conroy T, Hammel P, Hebbar M, Ben Abdelghani M, Wei AC, Raoul J-L, et al. FOLFIRINOX or gemcitabine as adjuvant therapy for pancreatic cancer. N Engl J Med 2018;379:2395–406. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
