

Eosinophilic features in clear cell renal cell carcinoma correlate with outcomes of immune checkpoint and angiogenesis blockade
- PMID: 34580162
- PMCID: PMC8477329
- DOI: 10.1136/jitc-2021-002922
Eosinophilic features in clear cell renal cell carcinoma correlate with outcomes of immune checkpoint and angiogenesis blockade
Abstract
Background: Clear cell renal cell carcinoma (ccRCC) displays heterogeneity in appearance-a distinctive pale clear to eosinophilic cytoplasm; however, little is known about the underlying mechanisms and clinical implications. We investigated the role of these eosinophilic features in ccRCC on oncological outcomes and response to tyrosine kinase inhibitors (TKIs) and immune checkpoint inhibitors (ICIs).
Methods: One-hundred and thirty-eight ccRCC cases undergoing radical surgery (cohort 1) and 54 metastatic ccRCC cases receiving either TKIs or ICIs (cohort 2) were included. After histological evaluation, all cases were divided into three phenotypes based on the eosinophilic features at the highest-grade area: clear, mixed, or eosinophilic type. Gene expression and immunohistochemical analyses were performed to explore the potential mechanisms of these phenotypes in cohort 1. Further, the association of the three phenotypes with the best objective response to TKI or ICI, clinical benefit (complete/partial response or stable disease), and overall survival (OS) was assessed in cohort 2.
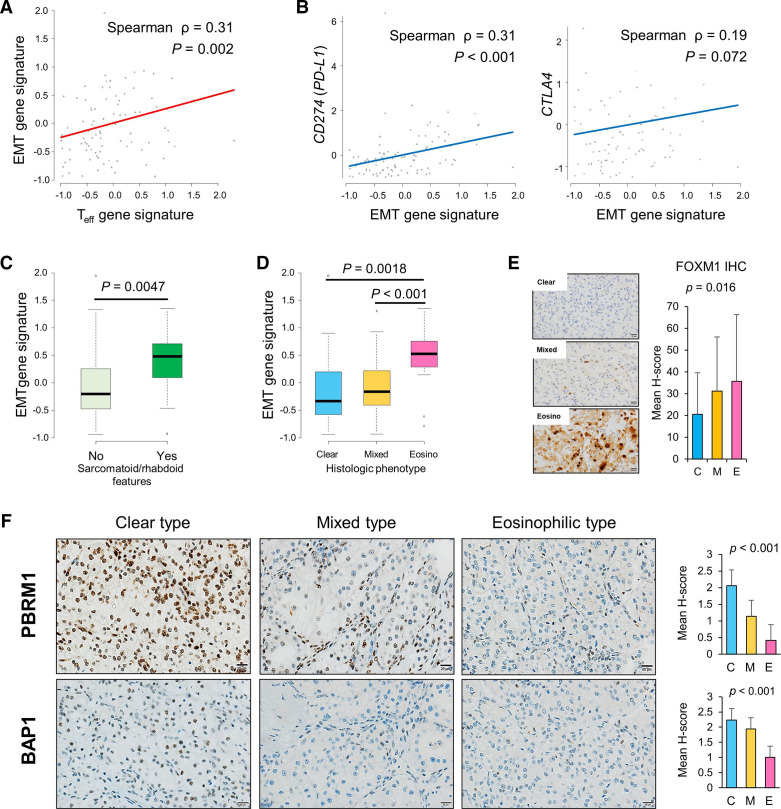
Results: The clear type was significantly associated with increased hypoxia as well as angiogenesis gene signatures compared with the eosinophilic type. Gene signatures and protein expression related to effector T cell and immune checkpoint molecules were elevated to a greater extent in the eosinophilic type, followed by the mixed and clear types. The mixed and eosinophilic types exhibited greater PBRM1-negativity and increased prevalence of the epithelial-mesenchymal transition gene signature than the clear type. In the mixed/eosinophilic types of cohort 2, significant clinical benefit was observed in the ICI therapy group versus the TKI therapy group (p=0.035), and TKI therapy vs ICI therapy was an independent factor for worse prognosis of OS (HR 3.236; p=0.012).
Conclusion: The histological phenotype based on the eosinophilic features, which are linked to major immunological mechanisms of ccRCC, was significantly correlated with therapeutic efficacy.
Keywords: biomarkers; immunohistochemistry; immunotherapy; kidney neoplasms; neovasularization; pathologic; tumor.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous