

This is a preprint.
Functional antibody and T-cell immunity following SARS-CoV-2 infection, including by variants of concern, in patients with cancer: the CAPTURE study
- PMID: 34580668
- PMCID: PMC8475970
- DOI: 10.21203/rs.3.rs-916427/v1
Functional antibody and T-cell immunity following SARS-CoV-2 infection, including by variants of concern, in patients with cancer: the CAPTURE study
Update in
-
Functional antibody and T cell immunity following SARS-CoV-2 infection, including by variants of concern, in patients with cancer: the CAPTURE study.Nat Cancer. 2021 Dec;2(12):1321-1337. doi: 10.1038/s43018-021-00275-9. Epub 2021 Oct 27. Nat Cancer. 2021. PMID: 35121900
Abstract
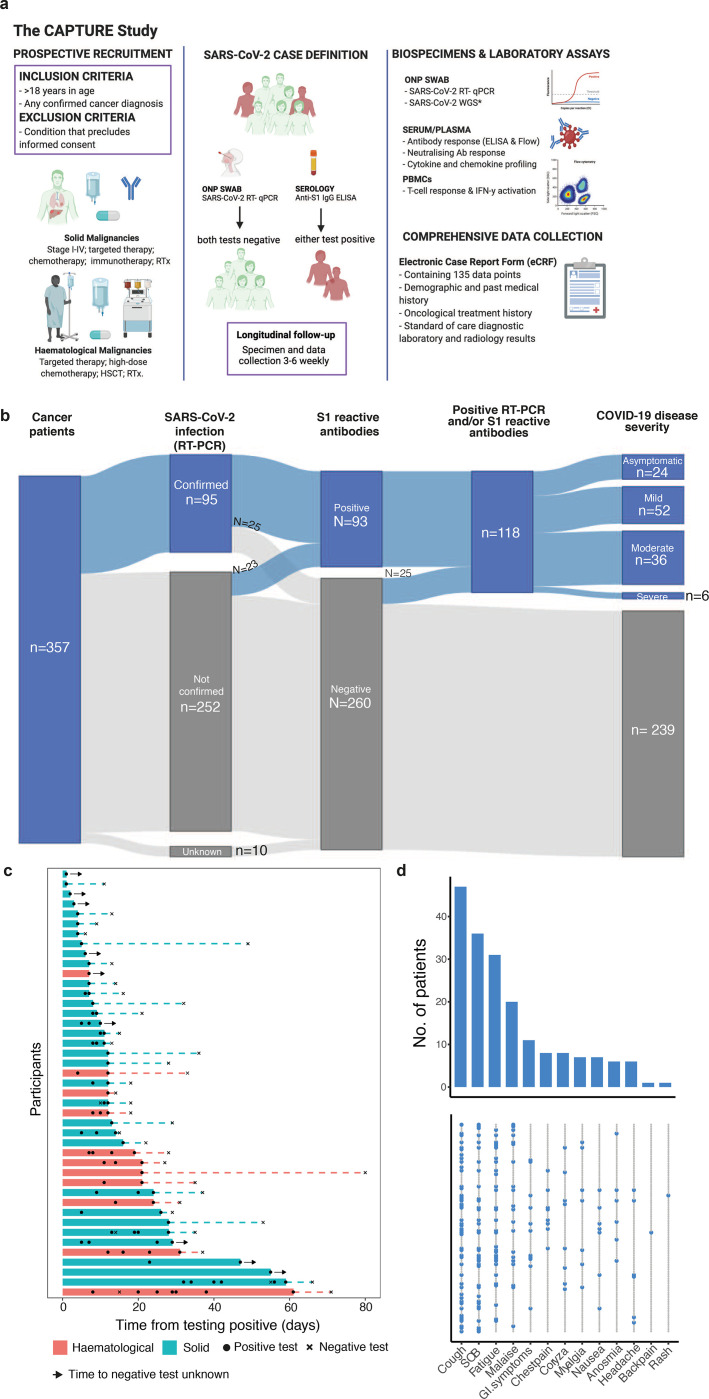
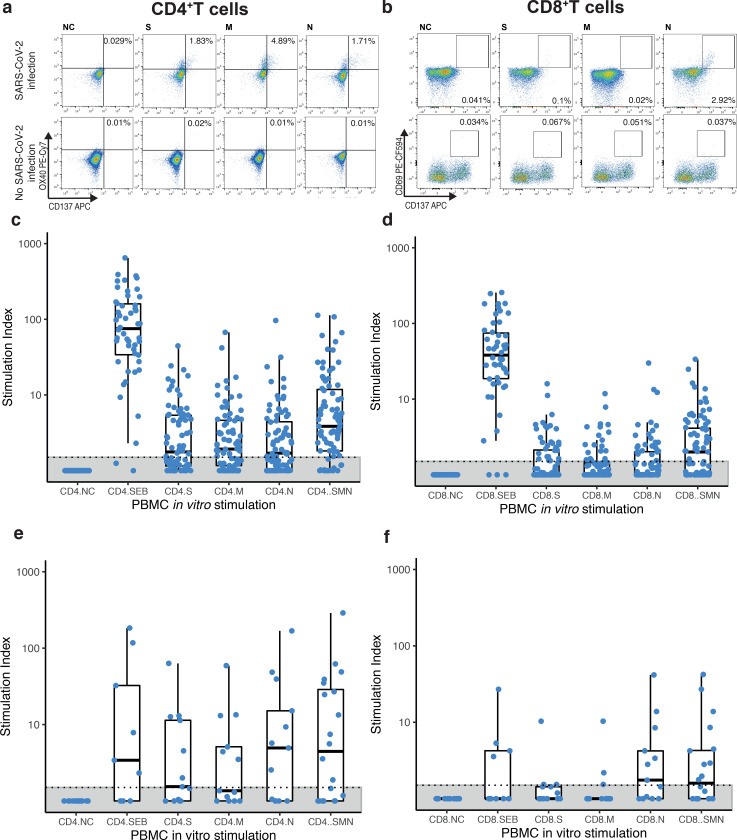
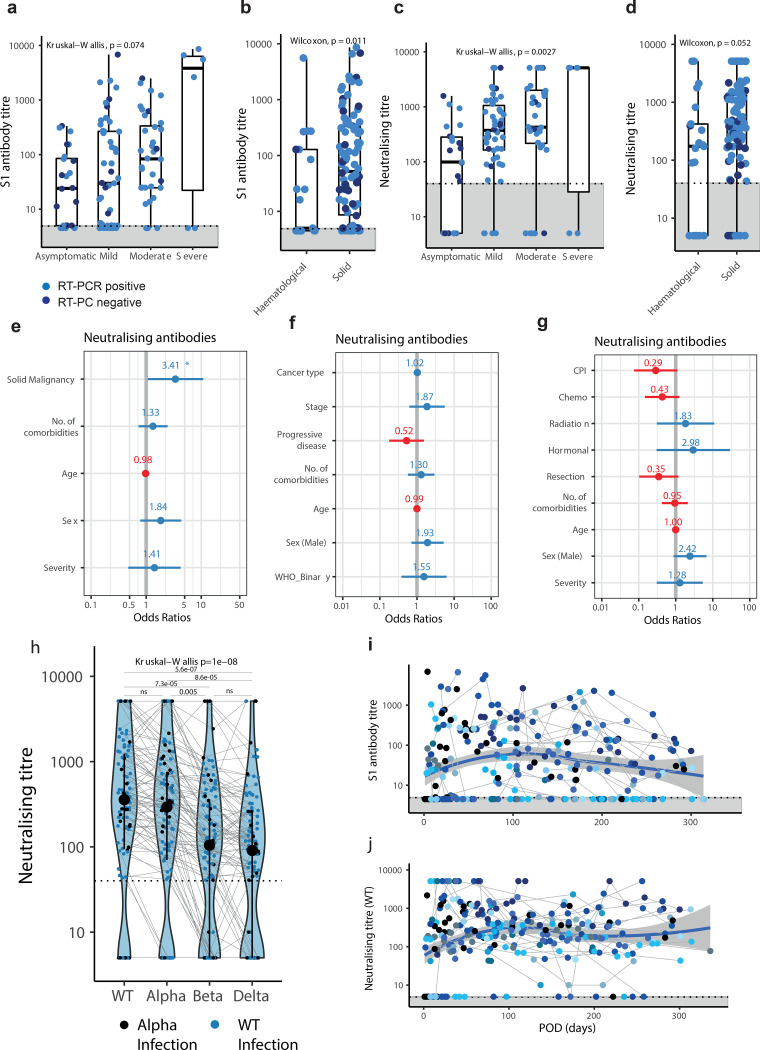
Patients with cancer have higher COVID-19 morbidity and mortality. Here we present the prospective CAPTURE study (NCT03226886) integrating longitudinal immune profiling with clinical annotation. Of 357 patients with cancer, 118 were SARS-CoV-2-positive, 94 were symptomatic and 2 patients died of COVID-19. In this cohort, 83% patients had S1-reactive antibodies, 82% had neutralizing antibodies against WT, whereas neutralizing antibody titers (NAbT) against the Alpha, Beta, and Delta variants were substantially reduced. Whereas S1-reactive antibody levels decreased in 13% of patients, NAbT remained stable up to 329 days. Patients also had detectable SARS-CoV-2-specific T cells and CD4+ responses correlating with S1-reactive antibody levels, although patients with hematological malignancies had impaired immune responses that were disease and treatment-specific, but presented compensatory cellular responses, further supported by clinical. Overall, these findings advance the understanding of the nature and duration of immune response to SARS-CoV-2 in patients with cancer.
Figures


References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
