Efficacy and safety of finerenone in patients with chronic kidney disease and type 2 diabetes by GLP-1RA treatment: A subgroup analysis from the FIDELIO-DKD trial
- PMID: 34580995
- PMCID: PMC9293162
- DOI: 10.1111/dom.14558
Efficacy and safety of finerenone in patients with chronic kidney disease and type 2 diabetes by GLP-1RA treatment: A subgroup analysis from the FIDELIO-DKD trial
Abstract
Aims: Finerenone significantly reduced the risk of kidney and cardiovascular (CV) outcomes in patients with chronic kidney disease and type 2 diabetes in the FIDELIO-DKD trial (NCT02540993). This exploratory subgroup analysis investigates the effect of glucagon-like peptide-1 receptor agonist (GLP-1RA) use on the treatment effect of finerenone.
Materials and methods: Patients with type 2 diabetes, urine albumin-to-creatinine ratio (UACR) 30-5000 mg/g and estimated glomerular filtration rate 25-<75 ml/min per 1.73 m2 receiving optimized renin-angiotensin system blockade were randomized to finerenone or placebo.
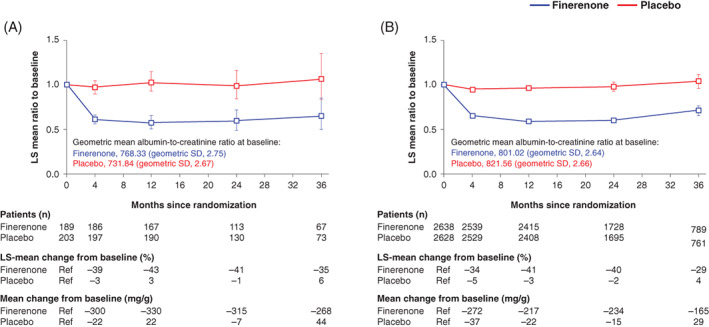
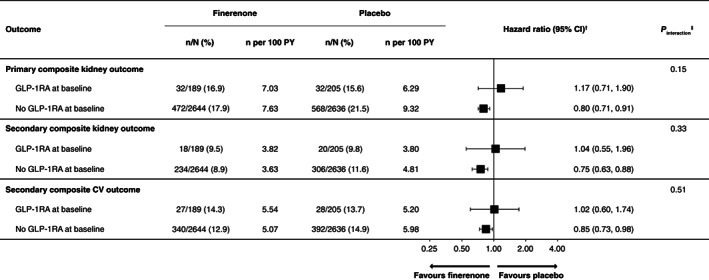
Results: Of the 5674 patients analysed, overall, 394 (6.9%) received GLP-1RAs at baseline. A reduction in UACR with finerenone was observed with or without baseline GLP-1RA use; ratio of least-squares means 0.63 (95% confidence interval 0.56, 0.70) with GLP-1RA use and 0.69 (95% confidence interval 0.67, 0.72) without GLP-1RA use (p value for interaction .20). Finerenone also significantly reduced the primary kidney (time to kidney failure, sustained decrease in estimated glomerular filtration rate ≥40% from baseline, or renal death) and key secondary CV outcomes (time to CV death, non-fatal myocardial infarction, non-fatal stroke, or hospitalization for heart failure) versus placebo, with no clear difference because of GLP-1RA use at baseline (p value for interaction .15 and .51 respectively) or any time during the trial. The safety profile of finerenone was similar between subgroups.
Conclusions: This exploratory subgroup analysis suggests that finerenone reduces UACR in patients with or without GLP-1RA use at baseline, and the effects on kidney and CV outcomes are consistent irrespective of GLP-1RA use.
Keywords: chronic kidney disease; finerenone; glucagon-like peptide-1 receptor agonist; mineralocorticoid receptor antagonist; type 2 diabetes.
© 2021 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
PR reports personal fees from Bayer, during the conduct of the study; he has received research support and personal fees from AstraZeneca and Novo Nordisk, and personal fees from Eli Lilly and Company, Boehringer Ingelheim, Astellas Pharma Inc., Gilead, Merck, Merck Sharp and Dohme, Mundipharma, Sanofi and Vifor Pharma. All fees are given to Steno Diabetes Center Copenhagen. RA reports personal fees and non‐financial support from Bayer Healthcare Pharmaceuticals Inc., during the conduct of the study; he also reports personal fees and non‐financial support from Akebia Therapeutics, Janssen, Relypsa Inc., Vifor Pharma, Boehringer Ingelheim, Sanofi, Eli Lilly and Company, AstraZeneca and Fresenius; he has received personal fees from Ironwood Pharmaceuticals, Merck & Co., Lexicon and Reata Pharmaceuticals, and non‐financial support from Otsuka America Pharmaceutical Inc., OPKO Health, Inc. and E. R. Squibb & Sons; he is a member of data safety monitoring committees for Amgen, AstraZeneca, and Celgene; a member of steering committees of randomized trials for Akebia Therapeutics, Bayer, Janssen and Relypsa Inc.; a member of adjudication committees for AbbVie, Bayer, Boehringer Ingelheim and Janssen; he has served as associate editor of the
Figures