

Troponin T in COVID-19 hospitalized patients: Kinetics matter
- PMID: 34581431
- PMCID: PMC8747831
- DOI: 10.5603/CJ.a2021.0104
Troponin T in COVID-19 hospitalized patients: Kinetics matter
Abstract
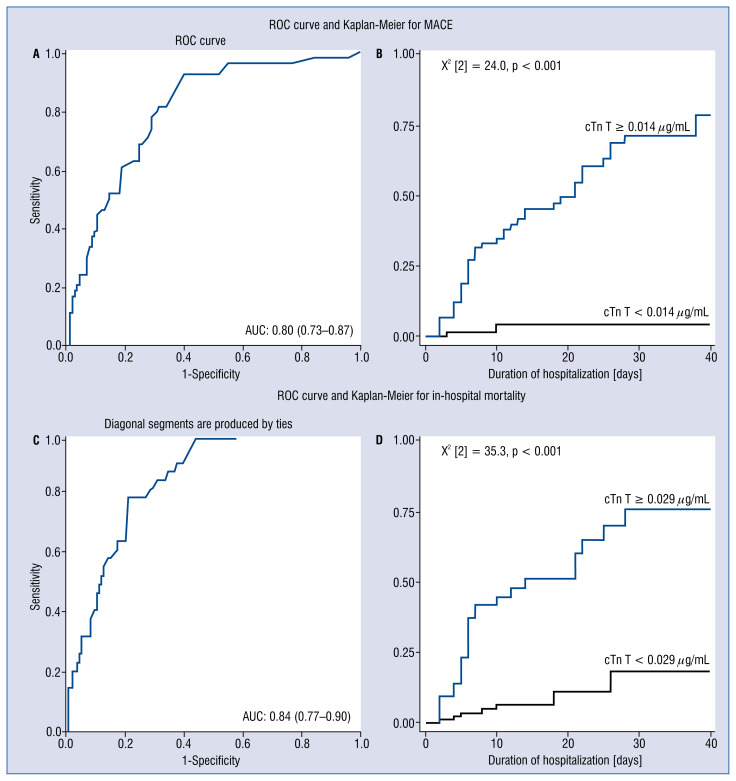
Background: Coronavirus disease 2019 (COVID-19) emerged as a worldwide health crisis, overwhelming healthcare systems. Elevated cardiac troponin T (cTn T) at admission was associated with increased in-hospital mortality. However, data addressing the role of cTn T in major adverse cardiovascular events (MACE) in COVID-19 are scarce. Therefore, we assessed the role of baseline cTn T and cTn T kinetics for MACE and in-hospital mortality prediction in COVID-19.
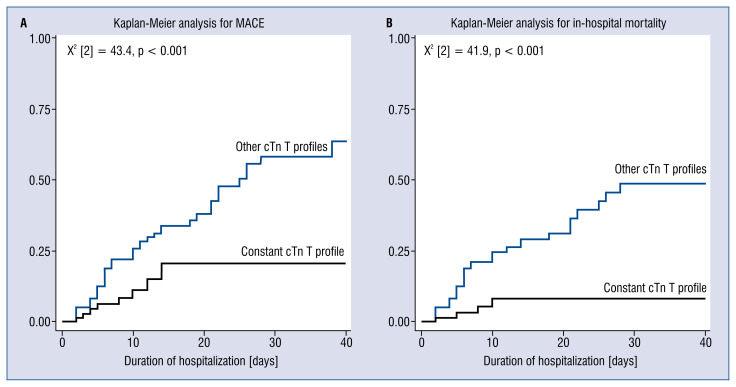
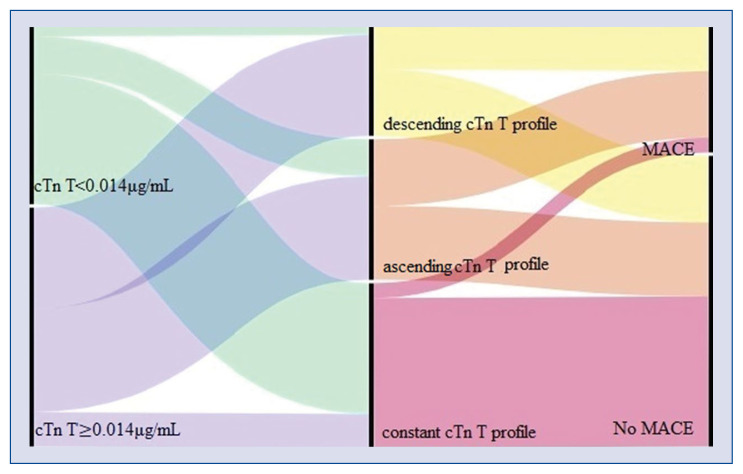
Methods: Three hundred and ten patients were included prospectively. One hundred and eight patients were excluded due to incomplete records. Patients were divided into three groups according to cTn T kinetics: ascending, descending, and constant. The cTn T slope was defined as the ratio of the cTn T change over time. The primary and secondary endpoints were MACE and in-hospital mortality.
Results: Two hundred and two patients were included in the analysis (mean age 64.4 ± 16.7 years, 119 [58.9%] males). Mean duration of hospitalization was 14.0 ± 12.3 days. Sixty (29.7%) patients had MACE, and 40 (19.8%) patients died. Baseline cTn T predicted both endpoints (p = 0.047, hazard ratio [HR] 1.805, 95% confidence interval [CI] 1.009-3.231; p = 0.009, HR 2.322, 95% CI 1.234-4.369). Increased cTn T slope predicted mortality (p = 0.041, HR 1.006, 95% CI 1.000-1.011). Constant cTn T was associated with lower MACE and mortality (p = 0.000, HR 3.080, 95% CI 1.914-4.954, p = 0.000, HR 2.851, 95% CI 1.828-4.447).
Conclusions: The present study emphasizes the additional role of cTn T testing in COVID-19 patients for risk stratification and improved diagnostic pathway and management.
Keywords: COVID-19; cardiac troponin; kinetics; major cardiovascular adverse events; mortality; myocardial injury.
Conflict of interest statement
Figures
References
-
- WHO. Aylward Bruce, (WHO), Liang W., (PRC) Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19) WHO-China Jt Mission Coronavirus Dis. 2019:2020.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
