

Effect of Thrombectomy With Combined Contact Aspiration and Stent Retriever vs Stent Retriever Alone on Revascularization in Patients With Acute Ischemic Stroke and Large Vessel Occlusion: The ASTER2 Randomized Clinical Trial
- PMID: 34581737
- PMCID: PMC8479584
- DOI: 10.1001/jama.2021.13827
Effect of Thrombectomy With Combined Contact Aspiration and Stent Retriever vs Stent Retriever Alone on Revascularization in Patients With Acute Ischemic Stroke and Large Vessel Occlusion: The ASTER2 Randomized Clinical Trial
Abstract
Importance: Mechanical thrombectomy using a stent retriever or contact aspiration is widely used for treatment of patients with acute ischemic stroke due to anterior circulation large vessel occlusion, but the additional benefit of combining contact aspiration with stent retriever is uncertain.
Objective: To determine whether mechanical thrombectomy for treatment of anterior circulation large vessel occlusion stroke with initial contact aspiration and stent retriever combined results in better final angiographic outcome than with standard stent retriever alone.
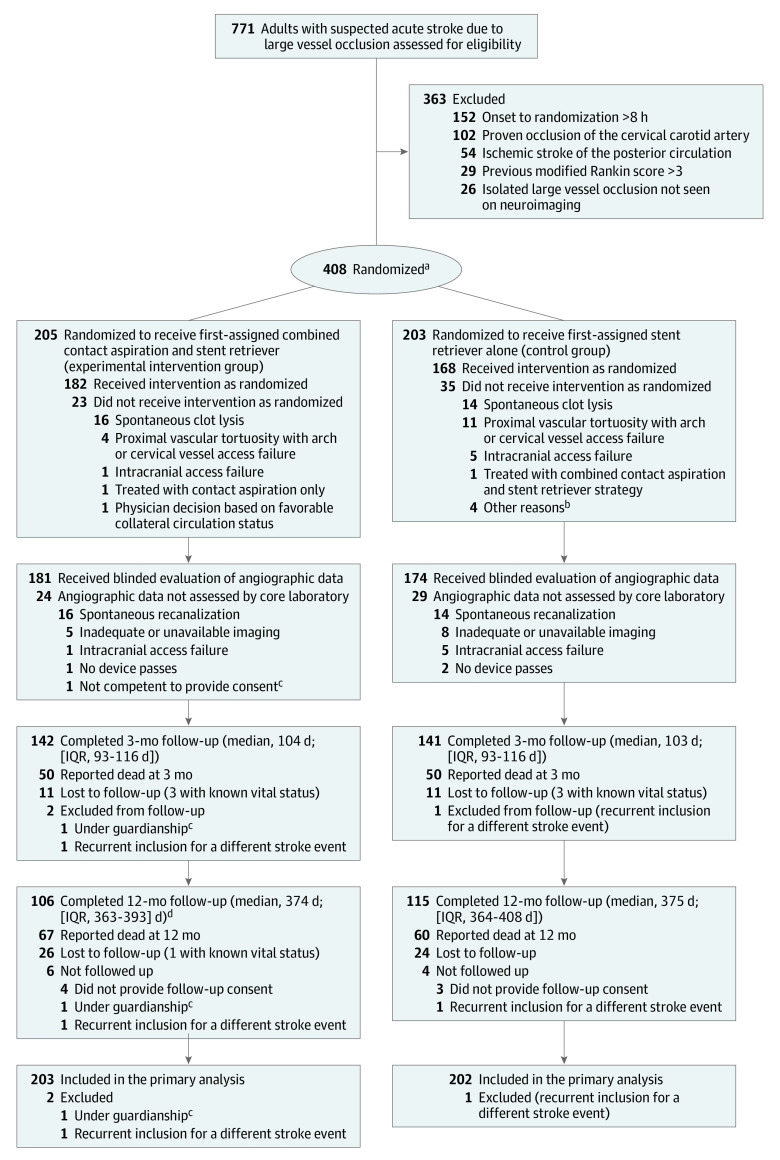
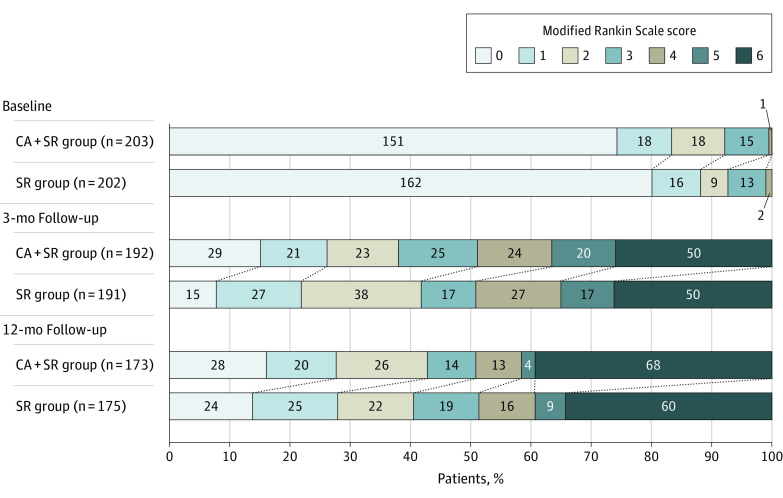
Design, setting, and participants: This trial was a multicenter randomized, open-label, blinded end point evaluation that enrolled 408 patients from October 16, 2017, to May 29, 2018, in 11 French comprehensive stroke centers, with a 12-month outcome follow-up. Patients with a large vessel occlusion in the anterior circulation were included up to 8 hours after symptom onset. The final date of follow-up was June, 19, 2019.
Interventions: Patients were randomly assigned (1:1 allocation) to receive initial thrombectomy with contact aspiration and stent retriever combined (205) or stent retriever alone (203).
Main outcomes and measures: The primary outcome was the rate of expanded Thrombolysis In Cerebral Infarction score of 2c or 3 (eTICI 2c/3; ie, scores indicate near-total and total reperfusion grades) at the end of the procedure.
Results: Among the 408 patients who were randomized, 3 were excluded, and 405 (99.3%) patients (mean age, 73 years; 220 [54%] women and 185 [46%] men) were included in the primary analysis. The rate of eTICI 2c/3 at the end of the endovascular procedure was not significantly different between the 2 thrombectomy groups (64.5% [131 of 203 patients] for contact aspiration and stent retriever combined vs 57.9% [117 of 202 patients] for stent retriever alone; risk difference, 6.6% [95% CI, -3.0% to 16.2%]; adjusted odds ratio [OR], 1.33 [95% CI, 0.88 to 1.99]; P = .17). Of 14 prespecified secondary efficacy end points, 12 showed no significant difference. A higher rate of successful reperfusion was achieved in the contact aspiration combined with stent retriever group vs the stent retriever alone group (eTICI 2b50/2c/3, 86.2% vs 72.3%; adjusted OR, 2.54 [95% CI, 1.51 to 4.28]; P < .001) and of near-total or total reperfusion (eTICI 2c/3, 59.6% vs 49.5%; adjusted OR, 1.52 [95% CI, 1.02 to 2.27]; P = .04) after the assigned initial intervention alone.
Conclusions and relevance: Among patients with acute ischemic stroke due to large vessel occlusion, an initial thrombectomy technique consisting of contact aspiration and stent retriever combined, compared with stent retriever alone, did not significantly improve the rate of near-total or total reperfusion (eTICI 2c/3) at the end of the endovascular procedure, although the trial may have been underpowered to detect smaller differences between groups.
Trial registration: ClinicalTrials.gov Identifier: NCT03290885.
Conflict of interest statement
Figures
References
-
- Turk AS III, Siddiqui A, Fifi JT, et al. Aspiration thrombectomy versus stent retriever thrombectomy as first-line approach for large vessel occlusion (COMPASS): a multicentre, randomised, open label, blinded outcome, non-inferiority trial. Lancet. 2019;393(10175):998-1008. doi: 10.1016/S0140-6736(19)30297-1 - DOI - PubMed
-
- Lapergue B, Blanc R, Gory B, et al. ; ASTER Trial Investigators . Effect of endovascular contact aspiration vs stent retriever on revascularization in patients with acute ischemic stroke and large vessel occlusion: the ASTER randomized clinical trial. JAMA. 2017;318(5):443-452. doi: 10.1001/jama.2017.9644 - DOI - PMC - PubMed
-
- Powers WJ, Rabinstein AA, Ackerson T, et al. ; American Heart Association Stroke Council . 2018 Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2018;49(3):e46-e110. doi: 10.1161/STR.0000000000000158 - DOI - PubMed
