

PD-1 inhibition in advanced myeloproliferative neoplasms
- PMID: 34581778
- PMCID: PMC9152999
- DOI: 10.1182/bloodadvances.2021005491
PD-1 inhibition in advanced myeloproliferative neoplasms
Abstract
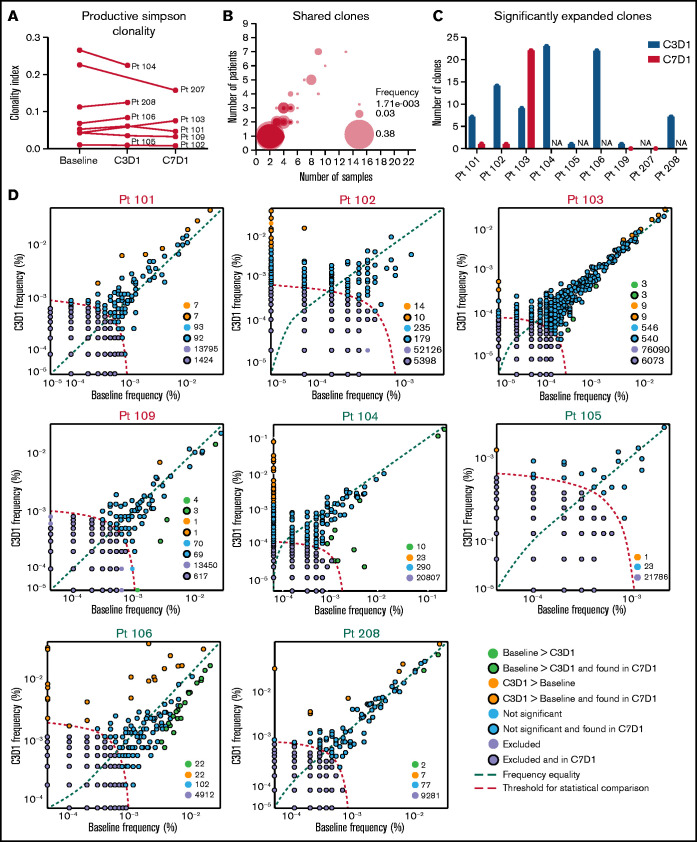
Myelofibrosis (MF) is a clonal stem cell neoplasm characterized by abnormal JAK-STAT signaling, chronic inflammation, cytopenias, and risk of transformation to acute leukemia. Despite improvements in the therapeutic options for patients with MF, allogeneic hematopoietic stem cell transplantation remains the only curative treatment. We previously demonstrated multiple immunosuppressive mechanisms in patients with MF, including increased expression of programmed cell death protein 1 (PD-1) on T cells compared with healthy controls. Therefore, we conducted a multicenter, open-label, phase 2, single-arm study of pembrolizumab in patients with Dynamic International Prognostic Scoring System category of intermediate-2 or greater primary, post-essential thrombocythemia or post-polycythemia vera myelofibrosis that were ineligible for or were previously treated with ruxolitinib. The study followed a Simon 2-stage design and enrolled a total of 10 patients, 5 of whom had JAK2V617mutation, 2 had CALR mutation, and 6 had additional mutations. Most patients were previously treated with ruxolitinib. Pembrolizumab treatment was well tolerated, but there were no objective clinical responses, so the study closed after the first stage was completed. However, immune profiling by flow cytometry, T-cell receptor sequencing, and plasma proteomics demonstrated changes in the immune milieu of patients, which suggested improved T-cell responses that can potentially favor antitumor immunity. The fact that these changes were not reflected in a clinical response strongly suggests that combination immunotherapeutic approaches rather than monotherapy may be necessary to reverse the multifactorial mechanisms of immune suppression in myeloproliferative neoplasms. This trial was registered at www.clinicaltrials.gov as #NCT03065400.
© 2021 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Figures




References
-
- Vannucchi AM, Lasho TL, Guglielmelli P, et al. Mutations and prognosis in primary myelofibrosis. Leukemia. 2013;27(9):1861-1869. - PubMed
-
- Barcellini W, Iurlo A, Radice T, et al. Increased prevalence of autoimmune phenomena in myelofibrosis: relationship with clinical and morphological characteristics, and with immunoregulatory cytokine patterns. Leuk Res. 2013;37(11):1509-1515. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
