

Prone Position in COVID-19 and -COVID-19 Acute Respiratory Distress Syndrome: An International Multicenter Observational Comparative Study
- PMID: 34582426
- PMCID: PMC8923275
- DOI: 10.1097/CCM.0000000000005354
Prone Position in COVID-19 and -COVID-19 Acute Respiratory Distress Syndrome: An International Multicenter Observational Comparative Study
Abstract
Objectives: Prone position is used in acute respiratory distress syndrome and in coronavirus disease 2019 acute respiratory distress syndrome. However, it is unclear how responders may be identified and whether an oxygenation response improves outcome. The objective of this study was to quantify the response to prone position, describe the differences between coronavirus disease 2019 acute respiratory distress syndrome and acute respiratory distress syndrome, and explore variables associated with survival.
Design: Retrospective, observational, multicenter, international cohort study.
Setting: Seven ICUs in Italy, United Kingdom, and France.
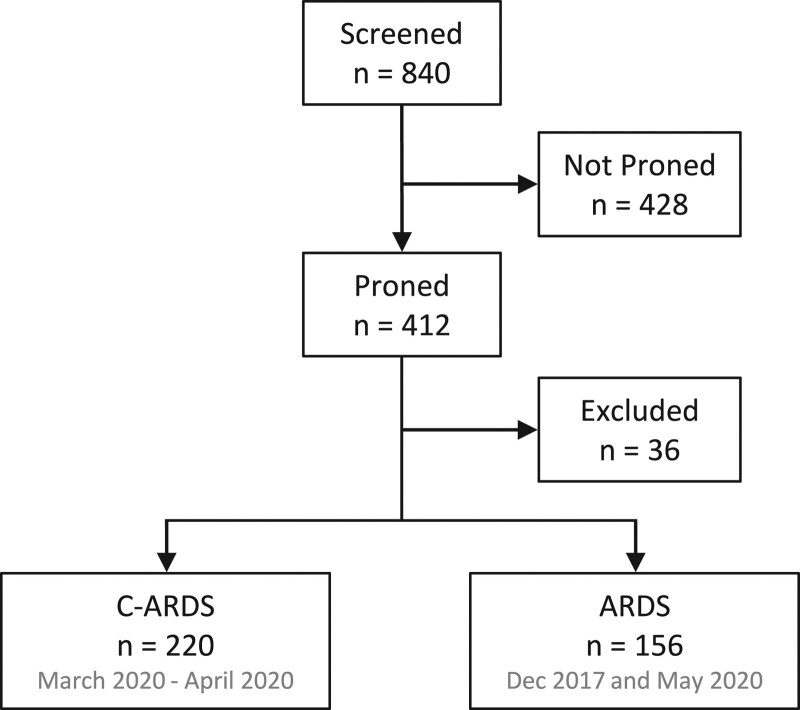
Patients: Three hundred seventy-six adults (220 coronavirus disease 2019 acute respiratory distress syndrome and 156 acute respiratory distress syndrome).
Intervention: None.
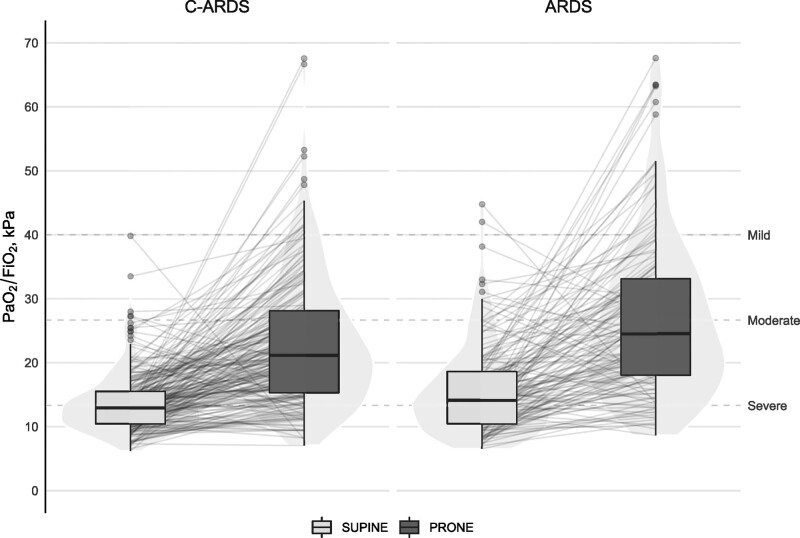
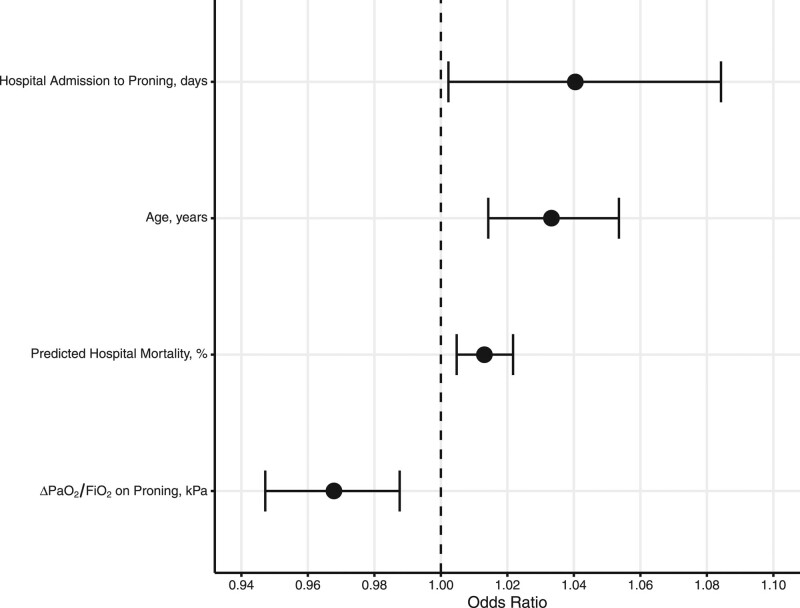
Measurements and main results: Preproning, a greater proportion of coronavirus disease 2019 acute respiratory distress syndrome patients had severe disease (53% vs 40%), worse Pao2/Fio2 (13.0 kPa [interquartile range, 10.5-15.5 kPa] vs 14.1 kPa [interquartile range, 10.5-18.6 kPa]; p = 0.017) but greater compliance (38 mL/cm H2O [interquartile range, 27-53 mL/cm H2O] vs 31 mL/cm H2O [interquartile range, 21-37 mL/cm H2O]; p < 0.001). Patients with coronavirus disease 2019 acute respiratory distress syndrome had a longer median time from intubation to prone position (2.0 d [interquartile range, 0.7-5.0 d] vs 1.0 d [interquartile range, 0.5-2.9 d]; p = 0.03). The proportion of responders, defined by an increase in Pao2/Fio2 greater than or equal to 2.67 kPa (20 mm Hg), upon proning, was similar between acute respiratory distress syndrome and coronavirus disease 2019 acute respiratory distress syndrome (79% vs 76%; p = 0.5). Responders had earlier prone position (1.4 d [interquartile range, 0.7-4.2 d] vs 2.5 d [interquartile range, 0.8-6.2 d]; p = 0.06)]. Prone position less than 24 hours from intubation achieved greater improvement in oxygenation (11 kPa [interquartile range, 4-21 kPa] vs 7 kPa [interquartile range, 2-13 kPa]; p = 0.002). The variables independently associated with the "responder" category were Pao2/Fio2 preproning (odds ratio, 0.89 kPa-1 [95% CI, 0.85-0.93 kPa-1]; p < 0.001) and interval between intubation and proning (odds ratio, 0.94 d-1 [95% CI, 0.89-0.99 d-1]; p = 0.019). The overall mortality was 45%, with no significant difference observed between acute respiratory distress syndrome and coronavirus disease 2019 acute respiratory distress syndrome. Variables independently associated with mortality included age (odds ratio, 1.03 yr-1 [95% CI, 1.01-1.05 yr-1]; p < 0.001); interval between hospital admission and proning (odds ratio, 1.04 d-1 [95% CI, 1.002-1.084 d-1]; p = 0.047); and change in Pao2/Fio2 on proning (odds ratio, 0.97 kPa-1 [95% CI, 0.95-0.99 kPa-1]; p = 0.002).
Conclusions: Prone position, particularly when delivered early, achieved a significant oxygenation response in ~80% of coronavirus disease 2019 acute respiratory distress syndrome, similar to acute respiratory distress syndrome. This response was independently associated with improved survival.
Copyright © 2022 by the Society of Critical Care Medicine and Wolters Kluwer Health, Inc. All Rights Reserved.
Conflict of interest statement
Dr. Terzi received funding from Pfizer. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Proning Responder or Not? This Is the Question.Crit Care Med. 2022 Apr 1;50(4):708-711. doi: 10.1097/CCM.0000000000005400. Crit Care Med. 2022. PMID: 34930861 Free PMC article. No abstract available.
References
-
- Guérin C, Reignier J, Richard JC, et al. ; PROSEVA Study Group: Prone positioning in severe acute respiratory distress syndrome. N Engl J Med 2013; 368:2159–2168 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
